
Clinical Presentation
Signs and Symptoms
 Polycystic Ovarian Syndrome_Initial Assesment 1
Polycystic Ovarian Syndrome_Initial Assesment 1
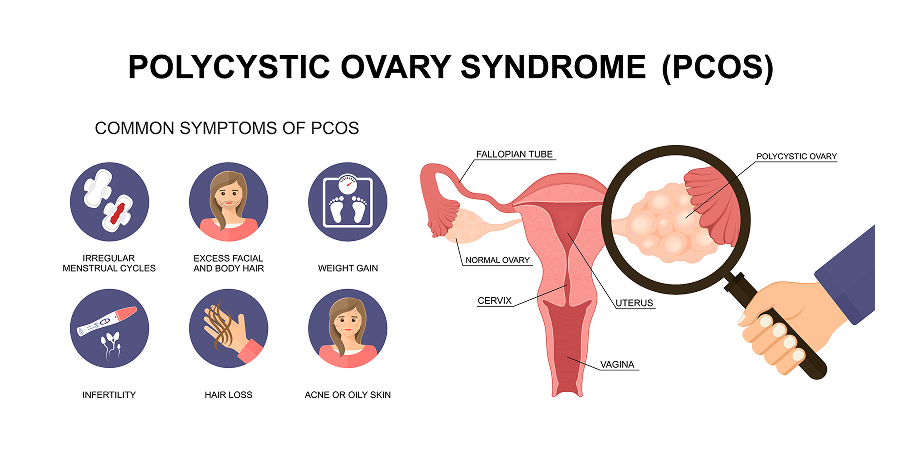
Hyperandrogenism
Hyperandrogenism may manifest clinically as: Hirsutism (excessive growth of hair on androgen-sensitive areas of the skin such as the chin, upper lip, sideburns, sternal, periareolar, umbilical, and sacral areas and more markedly on the pubic region and upper thighs); severe cystic and persistent acne; female-pattern hair loss (previously known as androgenetic alopecia); mild virilization; and rarely, male-pattern alopecia.
Reproductive Features
Reproductive
features in polycystic ovarian syndrome may clinically manifest as ovulatory
dysfunction or menstrual
disturbances, which include primary amenorrhea or secondary amenorrhea (ie the
absence of menses for >3 months after having had menses), oligomenorrhea,
dysfunctional uterine bleeding, anovulation, or infertility. Anovulatory
abnormal uterine bleeding may present as frequent bleeding at <21-day
intervals or infrequent bleeding at >35-day intervals. Pregnancy complications and endometrial cancer may also be
present.
Polycystic Ovaries
Polycystic ovaries are either ≥20 follicles measuring 2-9 mm in diameter or increased ovarian volume (OV) (>10 cm3).
Other Signs That May Be Present
Increased central adiposity and acanthosis nigricans are seen in Southeast Asians.
Obesity
Central visceral obesity is present in 35-80% of patients. Obesity is usually not as severe in women of Mediterranean descent, while BMI is lower in East Asians.
Hyperpigmentation
Hyperpigmentation may be found in skin fold creases. Acanthosis nigricans may also be observed in some patients.
Psychological
Features
Depression,
anxiety, eating disorders or poor quality of life may also be present in
polycystic ovarian syndrome.
History
 Polycystic Ovarian Syndrome_Initial Assesment 2
Polycystic Ovarian Syndrome_Initial Assesment 2Focus should be on the onset and duration of various signs of androgen excess, menstrual history, history of infertility, and concomitant medications (eg Valproic acid, exogenous androgens). Menstrual history must screen for the status of ovulation in women with polycystic ovarian syndrome seeking fertility. Virilizing signs with rapid onset and progression are unusual for polycystic ovarian syndrome and may indicate an ovarian or adrenal neoplasm. Family history of DM or CVD (especially first-degree relatives with premature onset of CVD) should be noted. Assess for OSA, eating disorder, and mood disorder. Consider the potential negative psychosocial impact on the patient of hyperandrogenism. Unwanted excess hair growth and/or alopecia reported by the patient should be considered important regardless of apparent clinical severity.
Physical Examination
Patients with polycystic ovarian syndrome usually have features of hyperandrogenism and chronic anovulation. Cutaneous symptoms of polycystic ovarian syndrome should be documented. Visual scales such as the modified Ferriman-Gallwey score (mFG) for hirsutism (level ≥4 to 6 indicating hirsutism, depending on ethnicity) and the Ludwig visual score for alopecia may be used during evaluation. Consider only terminal hairs for pathological hirsutism (untreated, >5 mm long, variable shape and texture, and pigmented). Though most cysts in polycystic ovarian syndrome are non-palpable, some ovarian cysts may be palpated as adnexal masses or swelling. Body mass index (BMI) and waist-hip ratio are calculated. Blood pressure (BP) should be checked at each clinic visit.
Diagnosis or Diagnostic Criteria
A woman with polycystic ovaries but without clinical symptoms does not meet criteria for polycystic ovarian syndrome.
Diagnosis of polycystic ovarian syndrome is based on the 2003 Rotterdam criteria:
- Two out of three of the following: Oligo-ovulation or anovulation (ovulatory dysfunction), clinical and/or biochemical hyperandrogenism, or polycystic ovaries on ultrasound
- Exclusion of other causes (congenital adrenal hyperplasia, androgen-secreting tumors, Cushing’s syndrome, thyroid disease, prolactinoma, or hyperprolactinemia)
The Androgen Excess-Polycystic
Ovary Syndrome Society guidelines criteria include clinical or
biochemical hyperandrogenism and at least one of the following: Polycystic
ovaries or oligo-ovulation or anovulation.
The presence of hirsutism should be considered predictive of biochemical hyperandrogenism and polycystic ovarian syndrome in adults. The presence of estrogen can be confirmed with a positive progesterone withdrawal test (Medroxyprogesterone is administered for 5 days, and withdrawal bleeding occurs if estrogen is present).