
Clinical Presentation
The clinical and sexual history and physical examination are important parts of the investigation.
Clinical Observations Associated with Vaginal Infections
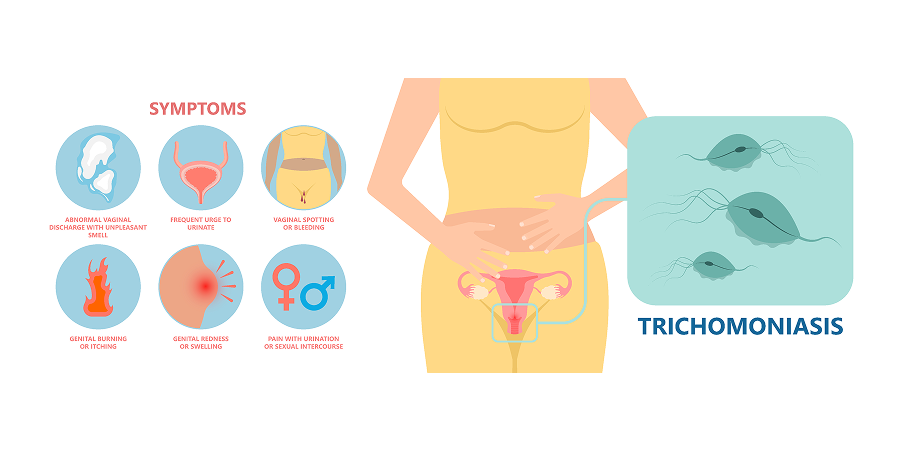
Trichomoniasis
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 1
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 1More than 50% of patients with trichomoniasis are asymptomatic or have minimal symptoms. Scanty to profuse, offensive vaginal discharge may be present. The patient may complain of vulval itching, dyspareunia, dysuria, and rarely, lower abdominal discomfort. A pelvic exam may reveal vulval erythema (“strawberry cervix”), vaginitis, cervicitis, vulvitis, or frothy, malodorous, greenish-yellow vaginal discharge pooled at the posterior fornix.
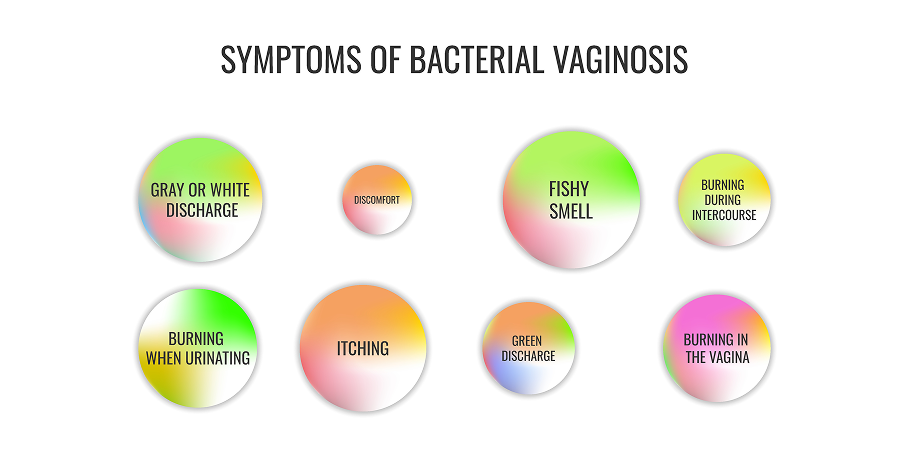
Bacterial Vaginosis (BV)
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 2
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 2Fifty percent of patients with bacterial vaginosis are asymptomatic. Thin discharge with a fishy or offensive odor may be present. A pelvic exam may reveal white or gray homogeneous discharge that coats the walls of the vagina and vestibule.
Vulvovaginal Candidiasis (VVC)
Ten to twenty percent of patients with vulvovaginal candidiasis are asymptomatic. The patient may complain of vulval itching and soreness, superficial dyspareunia, external dysuria, dyspareunia, and non-offensive vaginal discharge. A pelvic exam may show curdy (cottage cheese-like) vaginal discharge, satellite skin lesions, and, if severe vulvovaginal candidiasis is present, vulval erythema, fissuring, edema, and erosion may be observed.
History
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 3
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 3Inquire about characteristics of discharge (ie odor, onset [eg association with menstrual cycle], duration, color, and consistency); any associated symptoms (eg itch, dysuria, dyspareunia, abdominal pain, abnormal vaginal bleeding); and vulvovaginal hygiene practices (eg douching, shaving). Symptoms may vary as mixed vaginitis may occur (eg BV/VVC, BV/aerobic vaginitis [AV], VVC/AV). Assess the possible risk for sexually transmitted infections (ie <25 years old, new or multiple sexual partners, sexual behavior and practices, prior STIs, history of incarceration). Determine other comorbid conditions (eg diabetes mellitus [DM], immunocompromised states, inflammatory bowel disease), contraception use, and history of previous or current medication.
Physical Examination
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 4
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 4Perform a general assessment and look for signs of sexually transmitted infection. Examine mucocutaneous regions, including the pharynx. The external genitalia should be inspected for anatomical irregularities, cutaneous lesions, inflammation, and urethral discharge. Perianal inspection should be done. A digital rectal exam and anoscopy should be considered if the patient has practiced receptive anal intercourse or has rectal symptoms. Inguinal lymph nodes should be palpated. A vaginal swab should be obtained for a Gram stain and Trichomonas slide.
Illuminated Speculum Exam
Visualize the cervix and vaginal walls. Evaluate vaginal and endocervical vaginal discharges (ie consistency, amount, color, odor, and pH). Observe for cervical mucous, erosions, friability, foreign bodies, and growth. If resources are available, obtain specimens. A cervical swab should be obtained for Chlamydia test and gonorrhea culture.
Bimanual Pelvic Exam
Perform bimanual pelvic exam if upper genital tract infection is suspected. Detect uterine or adnexal masses, tenderness, or cervical motion tenderness. A finding of lower abdominal tenderness or cervical motion tenderness should prompt the attending physician to evaluate the patient for salpingitis and/or endometritis, which are part of pelvic inflammatory disease (PID). Treat the patient accordingly. Differential diagnoses may also include other surgical or gynecological conditions.
Please see Pelvic Inflammatory Disease disease management chart for further information.
Screening
Screening may be considered in asymptomatic women with risk factors (eg human immunodeficiency virus [HIV] infection) and/or those living in areas with high prevalence.
Human Immunodeficiency Virus (HIV) Testing and Counseling
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 5
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Initial Assesment 5
Human immunodeficiency virus (HIV) counseling and testing are recommended for trichomoniasis and bacterial vaginosis patients, unless other risk factors for HIV infection are identified. Bacterial vaginosis and T vaginalis are both associated with increased acquisition of HIV. Vulvovaginal candidiasis occurs more frequently and persistently in women with HIV, but the occurrence of recurrent VVC should not be an indication for HIV testing among women who previously tested HIV negative. Sexually transmitted infection (STI) consultation allows for an opportunity to discuss the patient's risk factors for sexually transmitted infections and HIV. Determine the patient’s risk for HIV and discuss HIV testing. Testing for HIV is recommended and should be offered to all persons seeking evaluation and treatment for sexually transmitted infections. Pretest and post-test counseling, as well as informed consent, are part of the testing procedure. Concomitant infection with HIV may complicate management and control of some sexually transmitted infections.