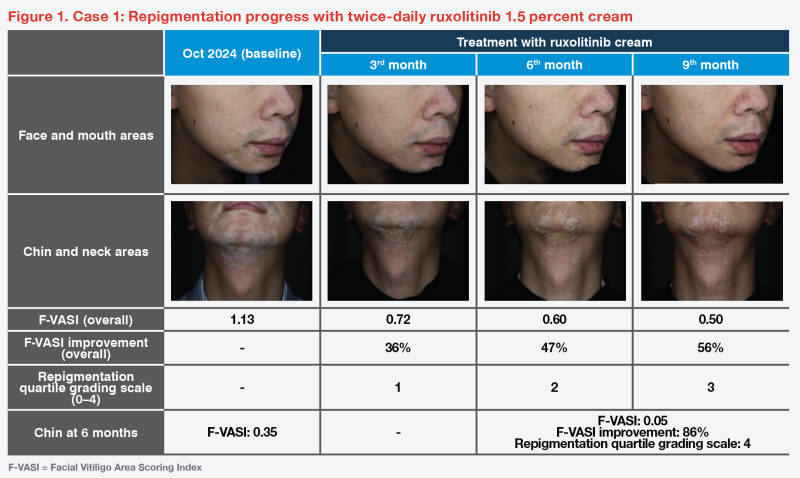
Case 1: Notable repigmentation with ruxolitinib cream in a patient with insufficient response to conventional treatments
A 37-year-old Chinese man with a 6-year history of vitiligo (onset at age of 25 years) first presented in November 2017 with extensive depigmentation over his nose, mouth, chin, forehead, back of his neck and hands, and the left elbow.
Treatment history included a topical calcineurin inhibitor (TCI; tacrolimus 0.1 percent) used in 2017–2024, narrow-band UVB (NB-UVB) in 2017–2021, and psoralen plus ultraviolet A (PUVA) therapy for the hands in 2020–2021. While facial lesions (especially over the central part of the face) persisted, other lesions showed marked improvement following treatment, especially after targeted phototherapy. (Figure 1)
In view of insufficient response to earlier treatments, twice-daily topical Janus kinase (JAK) inhibitor (ruxolitinib 1.5 percent) to the face and neck was initiated in October 2024.
Ruxolitinib treatment achieved notable improvements from baseline in the Facial Vitiligo Area Scoring Index (F-VASI) of 36 percent within 3 months and near-complete repigmentation within 9 months (in April 2025). (Figure 1)
The repigmentation achieved was maintained through September 2025 when the patient was last seen. He did not experience any side effects and is currently maintained on the same dose and schedule of ruxolitinib cream
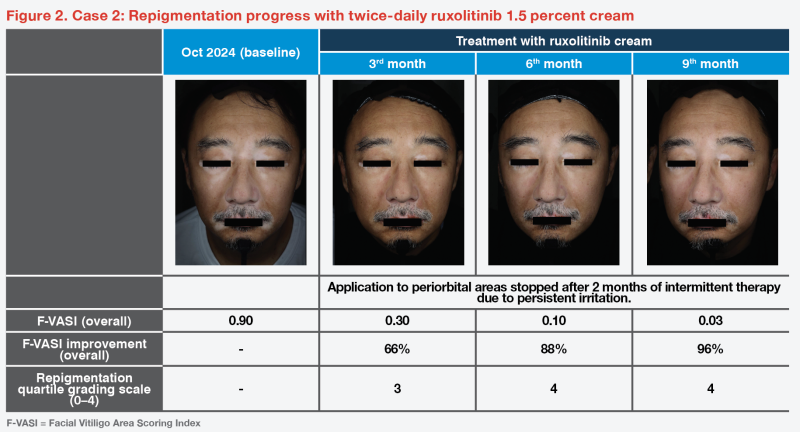
Case 2: Rapid and sustained repigmentation in a patient with unstable disease course
A 56-year-old Chinese man, with vitiligo onset at the age of 48 years, presented to our clinic in January 2018. Over the past year, he had progressive depigmentation over the central part of his face, periorificial area, hands, and back of his body. Further examination found more lesions on his heels and right elbow.
Treatment was initiated with tacrolimus 0.1 percent ointment for the eyelids, mometasone 0.1 percent cream for other parts of the face, and betamethasone 0.05 percent ointment for his back and hands. By May 2018, the patient had significant repigmentation over most of his face, especially the nose and eyelids. As the facial lesions had stabilized, mometasone application was stopped and replaced with tacrolimus ointment as maintenance therapy until September 2018.
In April 2019, new active facial lesions were treated with fluticasone 0.05 percent cream until January 2020. Other than minimal initial improvement, further response to TCI or topical corticosteroids was hardly visible. As phototherapy was not feasible due to his work commitments, the patient was advised to undergo sun exposure at home (by sunbathing on the balcony) starting August 2020, while continuing tacrolimus application. This resulted in improvement and stable repigmentation for approximately 1 year, before gradual depigmentation over the subsequent 3 years despite maintaining the same therapy.
Given the prolonged inadequate response to previous treatments, topical ruxolitinib was initiated in October 2024. The patient achieved a 66 percent improvement in F-VASI at 3 months, with near-complete repigmentation by 9 months in July 2025 (cumulative use: 60 g of ruxolitinib cream). Application to the periorbital region was discontinued after 2 months because of persistent conjunctival irritation (redness and tearing) despite intermittent cessations and rechallenges. Nonetheless, partial repigmentation of the periorbital areas was observed. (Figure 2)
When the patient was last seen in October 2025, repigmentation was largely maintained, with mild recurrence (slight depigmentation) around the right oral commissure. This was anticipated, given the patient’s historically unstable disease course. He remains on twice-daily ruxolitinib cream as maintenance therapy.
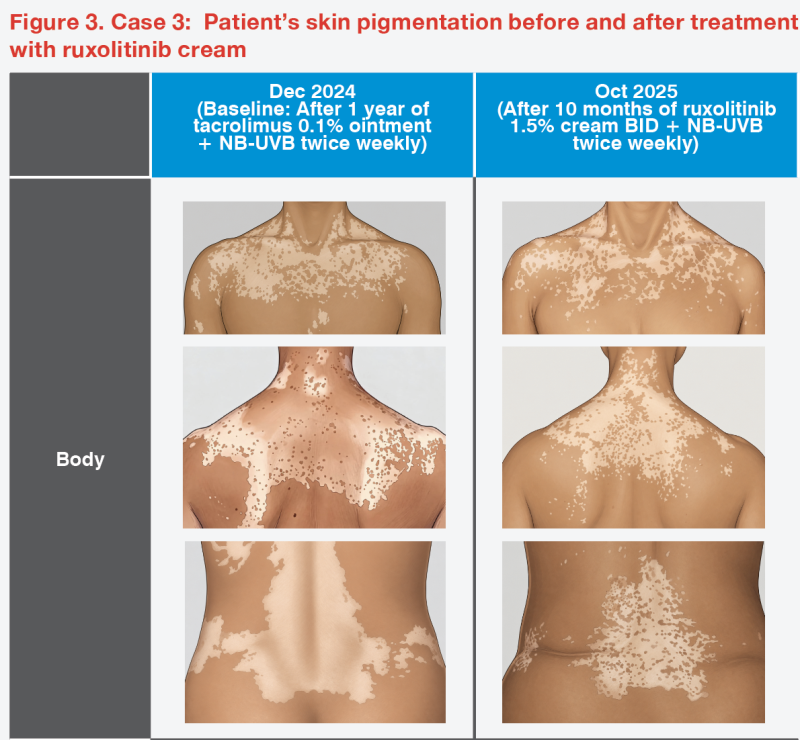
Case 3: Notable and ongoing improvements with phototherapy + ruxolitinib cream in a patient with extensive depigmentation
A 64-year-old woman with a 4-year history of vitiligo presented in July 2023 with very extensive depigmentation over her face, limbs, hands, and trunk. She also had a history of thyroid disease, a common comorbidity of vitiligo.
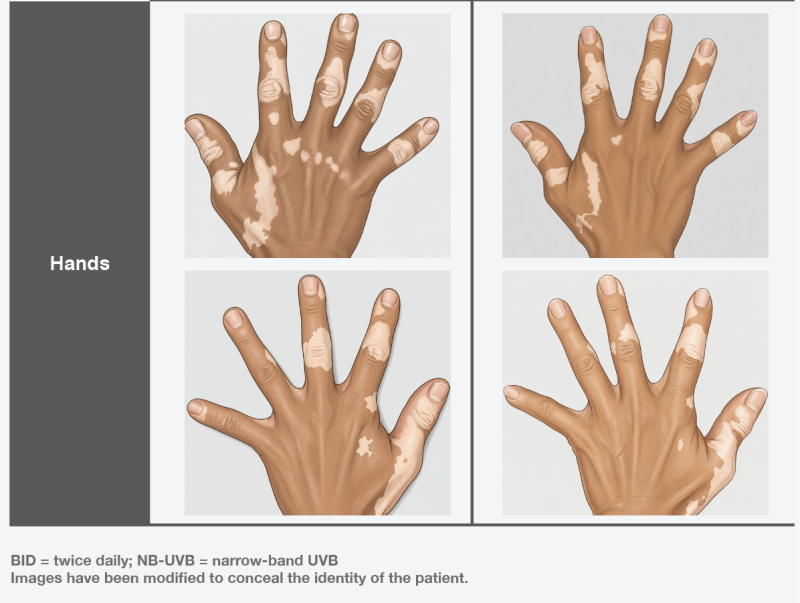
Prior to presentation, she had been treated with topical tacrolimus and corticosteroids, and advised to avoid sun exposure. In September 2023, twice-weekly NB-UVB phototherapy at initial UVB dose of 70 mJ/cm2 was started after minimal erythema dose (MED) testing, and the UVB dose was capped at around 1,700 mJ as tolerated. The phototherapy was combined with continued topical tacrolimus, resulting in some repigmentation after 1 year. As she desired further improvement, she was switched to topical ruxolitinib in December 2024 while maintaining NB-UVB therapy, leading to notable repigmentation after 10 months of combination therapy. (Figure 3)
Last seen in January 2026, the patient had further repigmentation, with ongoing improvement anticipated as she continues with dual therapy.
Discussion
Vitiligo is a chronic autoimmune disorder characterized by disfiguring skin depigmentation resulting from melanocyte loss. Conventional therapies are limited by modest and often unsustained efficacy, frequently disproportionate to the treatment burden borne by patients, necessitating more effective therapies.1,2 As seen in our patient cases, switching to an agent in a different therapeutic class (a topical JAK inhibitor) can result in clinically meaningful, significant, and sustained improvement with well-tolerated safety profile.
Interferon (IFN)-γ, which signals through the JAK1/JAK2-STAT1 pathway, plays a critical role in the pathogenesis of vitiligo, while interleukin (IL)-15 is an important cytokine that sustains resident memory T-cells, contributing to progression and recurrence/relapse of vitiligo. Ruxolitinib, a JAK1 and JAK2 inhibitor, reduces skin inflammation by selectively inhibiting STAT1 phophorylation, thereby reducing the IFN-γ driven inflammatory response and disrupting the positive feedback loop of melanocyte loss, thus facilitating endogenous repigmentation.1-3
Ruxolitinib cream is a first-in-class topical JAK inhibitor approved for the treatment of nonsegmental vitiligo with facial involvement in patients ≥12 years of age. Our patient cases reported above achieved F-VASI improvements of 86–96 percent within 9 months of therapy, consistent with the results of the two pivotal TRuE-V1 and TRuE-V2 studies, where ≥75 and ≥90 percent improvements in F-VASI (F-VASI75 and F-VASI90) at week 24 were achieved by significantly more patients treated with ruxolitinib 1.5 percent cream BID vs vehicle cream in both studies (F-VASI75: about 30 vs 10 percent; F-VASI90: 15– 16 vs 1–2 percent), with continued improvements sustained through week 52. Patients in these studies had a mean disease duration of ≥13 years and had received conventional treatments for many years, and a quarter of them had progressive disease.4-6
Among patients who achieved near-complete facial repigmentation (ie, F-VASI90) in TRuE-V1/V2 and continued treatment (n=58) in the roll-over TRuE-V long-term extension (LTE) study, about three in five maintained F-VASI75, and one in two maintained F-VASI90 at week 104.7 In the treatment-withdrawal arm (n=58) of the LTE study, repigmentation loss (<F-VASI90) occurred in half of the patients within 1 year of treatment withdrawal, with 44 percent losing repigmentation within 7 months. This underscores the importance of maintenance treatment after near-complete repigmentation is achieved with topical ruxolitinib.
Of patients who relapsed (<F-VASI75) after treatment withdrawal and restarted treatment in TRuE-V LTE, 75 percent regained F-VASI75 and approximately 70 percent regained F-VASI90.8
Patients with history of fluctuating/unstable disease course, such as case 2, may experience recurrence even with maintenance therapy during the immediate post-repigmentation period. With continued application of ruxolitinib cream, repigmentation returned. Hence, it is important to continue ruxolitinib twice-daily maintenance therapy until the disease reaches quiescent/stable state.
In the cohort of patients who entered the LTE study with <F-VASI90 (n=342), those with limited or no response at week 24 who continued ruxolitinib cream application for 80 more weeks generally had increased repigmentation.7,9 Hence, it is worthwhile for patients to persevere with treatment even if they do not see significant improvements within 6–9 months.
In my clinical experience, combination therapy with NB-UVB, such as in case 3, optimizes response and maximizes the efficacy of topical ruxolitinib by facilitating melanin production. This synergistic effect was seen in a subgroup of patients (n=19; 12/19 had not achieved F-VASI50 at week 24 with no substantial response after 6 months of monotherapy) who received concomitant NB-UVB phototherapy for >12 weeks during the open-label phase after a 52-week phase II study. Among these patients, 78.9 percent (15/19) and 94.7 percent (18/19) had improved F-VASI and total body (T)-VASI scores, respectively.10,11
Nevertheless, treatment of acral regions remains highly challenging due to lack of hair follicles and, hence, melanocytes in these areas. The slight improvement seen on the back of the hands of patient 3 could possibly be attributed to melanocyte cell migration from the unaffected areas.
Topical ruxolitinib is generally well tolerated. The most common side effects are irritation of the eyelid skin (one of the most sensitive areas of the face) and application-site acneiform eruptions.4 Persistent eye irritation, as observed in case 2, is uncommon. In most patients, treatment of sensitive facial areas can be continued following rechallenges after the irritation subsides, as initial local reactions typically diminish with repeated exposure. I typically advise a minimum of three rechallenges to patients to maximize chances of building tolerance.
As stated in a US Expert Consensus Statement on Use of Topical Therapeutics for Vitiligo in Pediatric, Adolescent and Young Adult Patients, topical JAK inhibitors (such as ruxolitinib cream) can be applied to areas with risk of atrophy including face, eyelids and groin, while risk of atrophy with long-term topical corticosteroid use is cautioned.11
Clinical responses to vitiligo therapy are typically delayed, with improvements often visible only several months after treatment initiation, as treatment success involves initial modulation and stabilization of immune dysregulation, followed by gradual repigmentation. Accordingly, proactive counselling is needed to help patients build realistic expectations of treatment outcomes, to ensure they are motivated to persevere with treatment.
Patients should be informed that repigmentation will most likely be imperfect and patchy, due to the natural distribution of hair follicles that serve as reservoirs for melanocyte regeneration. It is also worth mentioning that in clinical practice, repigmentation of approximately 50 percent relative to baseline is generally regarded as a meaningful/ significant therapeutic response.
Given the growing body of evidence supporting its efficacy and favourable tolerability profile, topical ruxolitinib may be considered as a first-line therapeutic option, particularly for patients with facial and neck involvement.
References:
- Dermatol Sin 2023;41:133-144.
- Annu Rev Immunol 2020;38:621-648.
- Lancet 2020;396:110-120.
- Lumirix Hong Kong Prescribing Information.
- www.fda.gov/drugs/news-events-human-drugs/fda-approves-topical-treatment-addressing-repigmentation-vitiligo-patients-aged-12-and-older.
- N Engl J Med 2022;387:1445-1455.
- Rosmarin D, et al, EADV 2024, poster P2984.
- Harris JE, et al, AAD 2023, abstract 46159.
- Wolkerstorfer A, et al, CDA 2024, poster 77.
- J Invest Dermatol 2022;142:3352-3355.
- JAMA Dermatol 2024;160:453-461.
This special report is supported by an education grant from the industry.
LUM/HKG/DOC-302/2026/rev.01