LDL-cholesterol (LDL-C) is the main driver of atherosclerotic cardiovascular disease (ASCVD), yet LDL-C control in high-risk patients remains far from optimal. At an industry-sponsored meeting, Professor Vivencio Barrios from Ramón y Cajal University Hospital, Spain, discussed the role of bempedoic acid in managing complex patients, while Dr Walter Wai-Chee Chen, Specialist in Cardiology in private practice in Hong Kong, shared local cases of bempedoic acid use in patients with mild-to-moderate chronic kidney disease (CKD) and complex clinical profiles.
Challenges of LDL-C control
In Asia, the burden of cardiovascular disease (CVD) has increased notably over the past decades, with high LDL-C rising from the 5th to the 4th leading modifiable CVD risk factor between 1990 and 2021. “Plaque builds up in the arteries over time and increases the risk of an acute cardiovascular [CV] event. Therefore, it is important to lower LDL-C as much as possible and as early as possible,” emphasized Barrios. [JACC Asia 2025:S2772-3747(25)00642-8; Nat Rev Cardiol 2024;21:701-716]
“However, in patients at high or very high CV risk, available lipid-lowering therapies [LLTs] are not being fully utilized, and combination therapy is particularly underused,” highlighted Barrios. In the THRESA study in Spain, even among patients receiving high-intensity statins, only 21.8 percent of high-risk patients and 28.3 percent of very high-risk patients achieved the recommended LDL-C targets. [Eur J Prev Cardiol 2021;28:1279-1289; Lancet Reg Health Eur 2023:29:100624; Eur Heart J 2020;41:111- 188; J Clin Med 2023;12:3187]
CLEAR Outcomes: Bempedoic acid
Bempedoic acid is a first-in-class, oral ATP-citrate lyase (ACL) inhibitor for LDL-C management. [Eur Heart J 2020;41:111-188] Its efficacy in statin-intolerant patients who had or were at high risk of CVD was demonstrated in the phase III CLEAR Outcomes trial. At 6 months, bempedoic acid effectively reduced mean LDL-C (-21.1 percentage points) and median high-sensitivity C-reactive protein (hs- CRP; -21.6 percentage points) vs placebo. After a median follow-up of 40.6 months, bempedoic acid significantly reduced the risks of first occurrence of four-component (hazard ratio [HR], 0.87; 95 percent confidence interval [CI], 0.79–0.96; p=0.004) and three-component major adverse cardiovascular events (MACE) (HR, 0.85; 95 percent CI, 0.76–0.96; p=0.006) vs placebo. [N Engl J Med 2023;388:1353-1364]
MILOS Germany: Bempedoic acid/ezetimibe FDC
MILOS is an ongoing European real-world study evaluating the use of bempedoic acid or bempedoic acid/ezetimibe fixed-dose combination (FDC) in adults with primary hypercholesterolaemia or mixed dyslipidaemia. “In the German cohort, >80 percent of patients received bempedoic acid in combination with other LLTs,” noted Barrios. At 2 years, LDL-C targets were reached in 35.3 percent of patients, compared with 4.9 percent before initiation of bempedoic acid or bempedoic acid/ezetimibe FDC treatment. [Clin Res Cardiol 2024;doi:10.1007/ s00392-024-02526-y] “Goal attainment increased by 26.9 percent in the high CV risk subgroup and 31.6 percent in the very high CV risk subgroup,” noted Barrios.
Bempedoic acid in patients with complex profiles
HK cases: Bempedoic acid in mild-to-moderate CKD
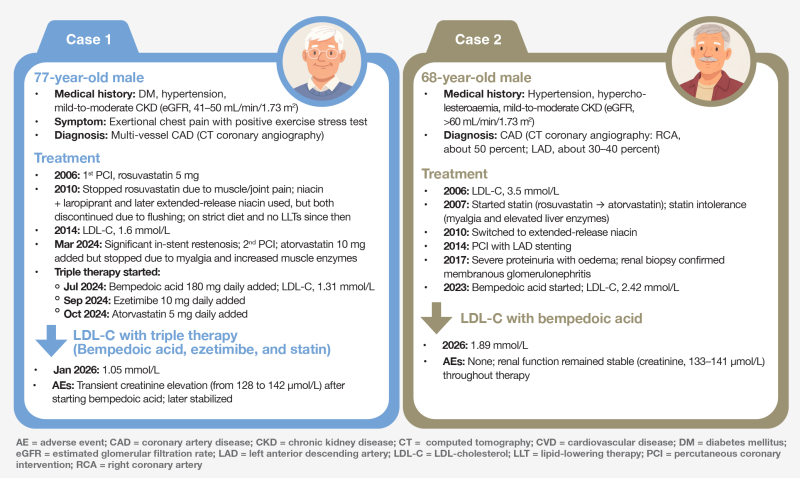
Two Hong Kong cases were presented to illustrate the use of bempedoic acid in patients with mild-to-moderate CKD and high CV risk who were reluctant to initiate proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitor therapy. In both cases, oral bempedoic acid reduced LDL‑C, either through combination therapy with ezetimibe and low‑dose statin (case 1) or as the primary oral strategy (case 2).
While fluctuations in creatinine levels may occur during treatment, these were transient and later stabilized in case 1. Renal function remained stable in case 2.
These two cases highlight the role of bempedoic acid in overcoming challenges in LDL‑C reduction among patients with high or very high CV risk.
DM & obesity
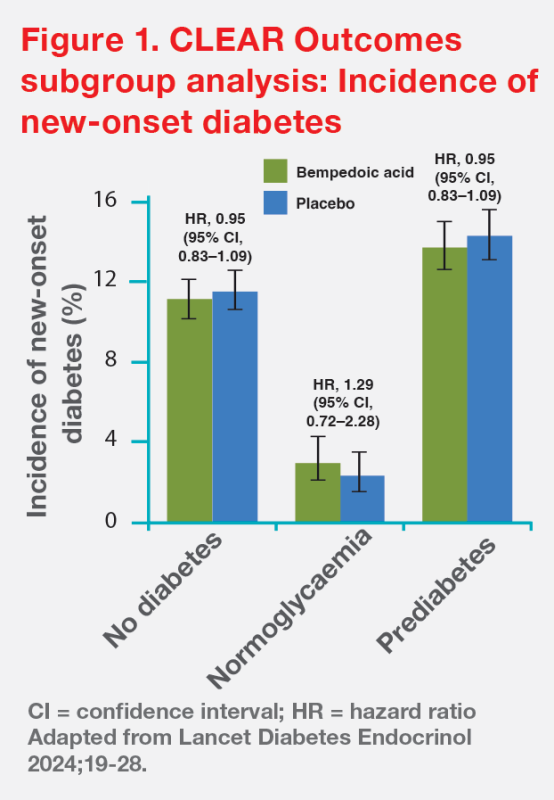
In a prespecified subgroup analysis of CLEAR Outcomes, bempedoic acid reduced LDL-C and the risk of four-component MACE in patients with or without diabetes mellitus (DM). Relative risk reductions in patients with DM, pre-DM and normoglycaemia were similar. Importantly, after a median of follow-up of 3.4 years, there was no significant increase in new-onset DM in patients treated with bempedoic acid. (Figure 1) Safety profiles were consistent across all glycaemic states. [Lancet Diabetes Endocrinol 2024;12:19-28]
Among patients with BMI >30 kg/ m2 in CLEAR Outcomes, bempedoic acid reduced four-component MACE (HR, 0.77) over a median follow-up of 40.7 months, and reduced LDL-C (-22.5 percent) and hs-CRP (-23.2 percent) at 6 months, with a safety profile consistent with previous reports. [J Am Heart Assoc 2025;14:e037898]
“In complex patients with mild-to-moderate CKD, DM, or obesity, bempedoic acid is a valuable option to help achieve good LDL-C control,” commented Barrios.
Role of bempedoic acid as an oral LLT
The 2025 Focused Update of the 2019 European Society of Cardiology (ESC)/European Atherosclerosis Society (EAS) guidelines support the use of bempedoic acid as monotherapy and in combination with other LLTs, emphasizing its key role in LDL-C control. [Eur Heart J 2025;46:4359-4378]
Bempedoic acid is recommended by ESC/EAS guidelines for statin-intolerant patients to achieve LDL-C goals (class I, level B). For high- or very high-risk patients already on maximally tolerated statin with or without ezetimibe, addition of bempedoic acid should be considered (class IIa, level C).
When to use bempedoic acid?
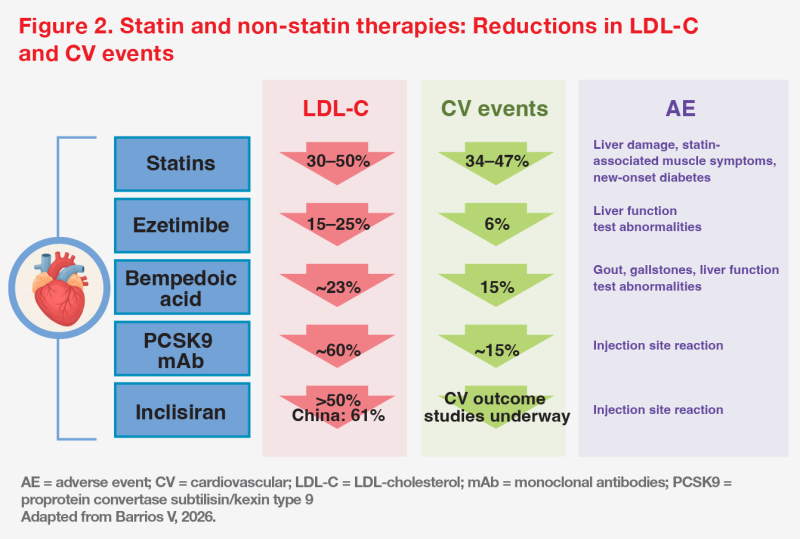
“Comparing the results of studies evaluating statins and non-statins, bempedoic acid demonstrated strong performance in reducing both LDL‑C and CV events,” said Barrios. (Figure 2)
“When used with high-intensity statin therapy, bempedoic acid reduces LDL-C to levels similar to those achieved with PCSK9 inhibitors. These two options, however, differ substantially in cost and patients’ acceptance,” stated Barrios. [Eur Heart J 2025;46:4359-4378] “When selecting a non-statin agent to manage LDL-C, patients are often reluctant to consider injectable therapies such as PCSK9 inhibitors due to cost or needle phobia.”
“Notably, bempedoic acid and PCSK9 inhibitors showed similar reductions in CV events [about 15 percent] in clinical trials, despite differences in LDL-C lowering,” Barrios added. (Figure 2) “The CV benefits of bempedoic acid make it a practical option for patients unwilling to receive injections.” [J Am Heart Assoc 2025;14:e044134; Curr Probl Cardiol 2024;49:102637]
“The best candidates for bempedoic acid treatment are patients who do not achieve LDL-C targets with prior therapies, regardless of the prior agents used,” Barrios said. “In complex patients with ASCVD, familial hypercholesterolaemia or statin intolerance, bempedoic acid plays an important role in helping to control LDL-C as effectively as possible.” [Arch Med Sci 2022;18:1429-1434]
Well-tolerated safety profile
Bempedoic acid is activated only in the liver, making it less likely to cause muscle-related adverse events commonly associated with statins. It was generally well tolerated in special populations, including patients with mild-to-moderate renal impairment, who require no dose adjustment. [JAMA Cardiol 2024;9:245-253; Nilemdo Hong Kong Prescribing Information]
Although bempedoic acid is associated with a higher incidence of gout in patients with elevated baseline uric acid, the use of uric acid–lowering therapy either before starting bempedoic acid or after a first gout event can reduce the rates of gout. [JACC Adv 2025;4:102207]
“Given its CV benefits, bempedoic acid should not be discontinued due to increases in uric acid,” suggested Barrios. “Instead, baseline uric acid should be assessed and managed with uric acid–lowering therapy as needed.”
Summary
Patients with complex clinical profiles, including those with mild-to-moderate CKD, DM, obesity, or statin intolerance, face multiple challenges in achieving LDL-C targets. Bempedoic acid is an effective oral, non-statin option, either as monotherapy or in combination with other LLTs, for reducing both LDL-C and CV events, with consistent benefits and a favourable tolerability profile observed across high-risk populations. For patients who are unable or reluctant to use injectable therapies, bempedoic acid is a practical option, supported by its proven benefits in preventing CV events.
This special report is supported by an education grant from the industry.
Approval code: HK-DAI-NN-2604029
Approval date: May 2026