Presentation, medical history and initial treatment
An 82-year-old retired physician with multiple cardiovascular (CV) risk factors presented with heart failure (HF). His medical history included hypertension, diabetes mellitus, hyperlipidaemia, and stage 4 chronic kidney disease (CKD) with estimated glomerular filtration rate (eGFR) of 25 mL/min/1.73 m2 and creatinine level of 350 μmol/L. Despite these comorbidities, he was enjoying a good quality of life and had recently been on a cruise.
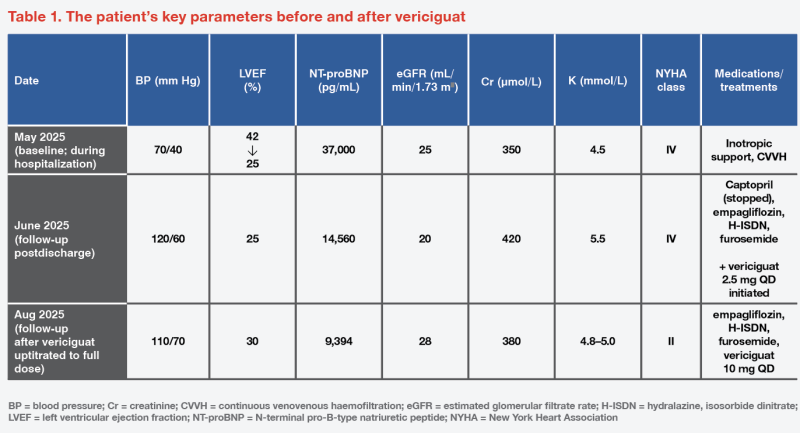
He underwent pacemaker implantation for 2:1 atrioventricular block in May 2025. Baseline echocardiography in May 2025 showed HF with mid-range ejection fraction (HFmrEF), with left ventricular ejection fraction (LVEF) of 42 percent and markedly elevated right ventricle systolic pressure (RVSP; 89 mm Hg). He was subsequently admitted with ischaemic pulmonary oedema complicated by cardiogenic shock, requiring inotropic support and continuous venovenous haemofiltration in the intensive care unit, where his LVEF dropped to 25 percent. (Table 1) Percutaneous coronary intervention was performed, and the patient was discharged after stabilization.
Follow-up management
At follow‑up, home blood pressure (BP) was approximately 120/60 mm Hg, and functional status was New York Heart Association (NYHA) class IV. Standard guideline-directed medical therapy (GDMT) was limited by advanced renal dysfunction. Renin–angiotensin–aldosterone system (RAAS) blockade with captopril, even at low dose (6.25 mg BID), was stopped because of hyperkalaemia (potassium, 5.5 mmol/L) and creatinine elevation (420 μmol/L). Beta-blockers and ivabradine were contraindicated due to atrioventricular block and frequent ventricular pacing (DDD mode). Mineralocorticoid receptor antagonists (MRAs) were not used because eGFR was <30 mL/min/1.73 m2. He was therefore maintained on empagliflozin 10 mg QD, hydralazine 25 mg BID and isosorbide dinitrate 10 mg BID, with loop diuretic as required. (Table 1)
Vericiguat treatment and response
Given the limited GDMT options and persistent severe symptoms, vericiguat was initiated in June 2025 at 2.5 mg QD and uptitrated sequentially to 5 mg and then 10 mg QD alongside furosemide 40 mg QD. The patient declined cardiac resynchronization therapy–defibrillator upgrade owing to age.
At follow-up in August 2025, the patient’s LVEF had improved to 30 percent, N-terminal pro-B-type natriuretic peptide (NT-proBNP) decreased from 14,560 to 9,394 pg/mL, and functional status improved from NYHA functional class IV to II. Home BP was approximately 110/70 mm Hg. (Table 1) Vericiguat was well tolerated and associated with symptomatic and echocardiographic improvements despite persisting stage 4 CKD. The patient’s overall condition returned to prehospitalization state and he was able to undertake his regular activities of daily living.
Discussion
GDMT optimization and its challenges
Optimization of GDMT remains central to improving outcomes and reducing worsening events in HFrEF.1 RAAS antagonists, including angiotensin-converting enzyme inhibitors, angiotensin receptor blockers and angiotensin receptor–neprilysin inhibitor, together with MRAs, are core GDMT components, and GDMT intensification has been shown to reduce CV death and/ or HF hospitalization (HFH).2
The multinational, open-label, randomized STRONG-HF study (n=1,078) demonstrated that high-intensity care (GDMT uptitration to full recommended doses) reduced the composite of HF readmission or all-cause death at 180 days vs usual care (15.2 vs 23.3 percent; risk difference, 8.1 percent; p=0.0021) in patients hospitalized with acute HF. A sensitivity analysis excluding COVID-19 deaths showed a result that was consistent with these findings.3 Consequently, many hospitals now pursue high-intensity GDMT titration in the ambulatory or clinic setting to reduce HFH and CV mortality in HFrEF.
Despite this, full GDMT implementation or intensification is not always well tolerated, posing a major challenge in routine practice. In STRONG‑HF, 3 percent of patients receiving high-intensity care (vs 1 percent with usual care) had renal impairment, jeopardizing further GDMT uptitration or addition of core GDMT agents.3 Real‑world data from a Chinese cohort (n=110) found that the main reason for GDMT intolerance was renal insufficiency (41.8 percent). Compared with those who tolerated GDMT, GDMT‑intolerant patients had lower eGFR (50.4 vs 70.9 mL/min/1.73 m2; p=0.002), higher prevalence of CKD (56.4 vs 23.6 percent; p<0.001) and higher baseline NT‑proBNP.4
CKD and HF often coexist, creating a vicious circle of progressive cardiac and renal dysfunction and markedly worse prognosis.1,5 In a retrospective Chinese cohort (n=217), HFrEF patients with worsening renal function (eGFR ≤30 mL/min/1.73 m2) had a five-fold higher risk of three-point major adverse cardiac events at 1 year vs those with normal renal function (eGFR >60 mL/min/1.73 m2) (hazard ratio [HR], 5.13; p=0.021), as well as substantially lower 2-year survival (50 vs 93 percent).6
Renal function decline is also prognostic and may precede HFH or death by up to 1 year, linking to symptomatic congestion.7 Pooled analyses of clinical trials (EPHESUS and EMPHASIS-HF) and a real-world cohort (BARCELONA) showed steeper eGFR declines in the year before an HF-related event vs in patients without events (average, -4.83 vs -1.18 mL/min/1.73 m2/year). Similar renal function trajectories were observed in BARCELONA (-5.77 vs -1.35 mL/min/1.73 m2/year). Worsening NYHA class also paralleled steeper eGFR decline, supporting monitoring of eGFR trajectory rather than relying solely on specific cut-offs for early detection of at-risk patients.7
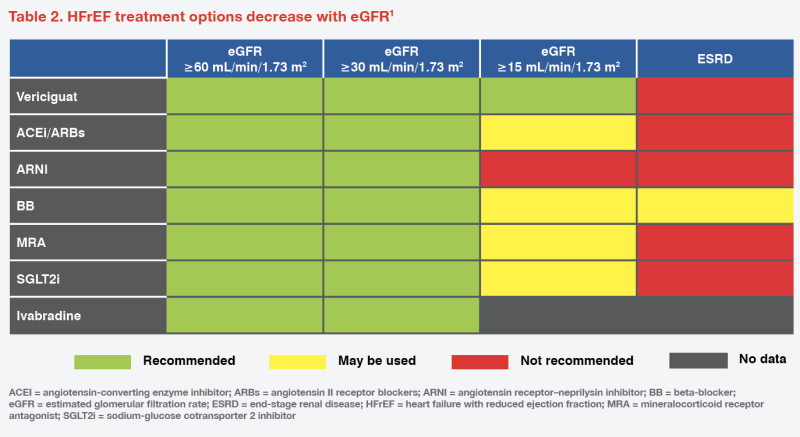
Although HFrEF patients with renal dysfunction require more intensive treatment due to worse prognosis, pivotal HFrEF randomized trials have historically excluded patients with stage 4 and 5 CKD, meaning therapeutic options for patients with eGFR <30 mL/min/1.73 m2 are limited.1 (Table 2) Notably, RAAS antagonists, ARNI and MRAs require renal and electrolyte monitoring and are frequently limited by reduced eGFR or hyperkalaemia.2 There are also restrictions for sodium-glucose cotransporter-2 inhibitor (SGLT2i) use when eGFR is <20–30 mL/min/1.73 m2.6,8 Hence, an unmet need persists for effective therapies that address residual risk in HFrEF patients with advanced CKD.2 This was exemplified by our patient for whom GDMT could not be optimized due to severe renal impairment, hyperkalaemia with specific agents, and concomitant conditions.
Vericiguat as a viable add-on to GDMT
Based on available literature, for patients with eGFR <30 mL/min/1.73 m2, such as our patient with eGFR <20 mL/min/1.73 m2, vericiguat is a viable add-on to suboptimally titrated GDMT.1
Vericiguat is an oral soluble guanylate cyclase (sGC) stimulator that kapag directly increases cyclic guanosine monophosphate (cGMP) production, stimulating the nitric oxide (NO)–sGC–cGMP pathway. In HF, oxidative stress and inflammation contribute to endothelial dysfunction in part through decreased NO availability, which leads to diminished sGC activity and cGMP production, precipitating myocardial and vascular dysfunction. Vericiguat both increases the sensitivity of sGC to NO activation and directly stimulates sGC activity, ameliorating the deficiency in cGMP, thereby improving cardiovascular function.9
In addition to strong efficacy data in HFrEF, vericiguat’s favourable safety profile makes it suitable for patients with CKD, in whom GDMT optimization may be challenging. In the phase III randomized VICTORIA trial (n=5,050), after a median follow-up of 10.8 months, vericiguat reduced the primary composite outcome of CV death or HFH by 10 percent vs placebo (HR, 0.90; 95 percent confidence interval, 0.83–0.98; p=0.02) in the overall population. The study included patients with eGFR of 15–30 mL/min/1.73 m2 whose proportion was capped at 15 percent.10 Importantly, the beneficial effect was not influenced by baseline eGFR and was similar in patients with or without early worsening of renal function (≥0.3 mg/ dL increase in creatinine from baseline to week 16).2
In a real-world cohort of 217 HFrEF patients initiated on vericiguat in hospital, mean LVEF improved significantly by 11.8 percent at 6 months (p<0.001). The subgroup with eGFR of ≤30 mL/min/1.73 m2 (n=31) showed the largest LVEF gain (20.2 percent; p=0.044), while the subgroup with eGFR >60 mL/min/1.73 m2 showed a less pronounced LVEF increase (10.9 percent; p<0.001).6
Vericiguat has a favourable safety profile and showed no excess of adverse events vs placebo in VICTORIA.5 Pooled analyses and real-world reports have not identified clinically meaningful effects on eGFR, serum creatinine, and sodium and potassium, making electrolyte monitoring unnecessary.2,11 Risks of symptomatic hypotension, renal and urinary disorders, and acute kidney injury were similar to placebo.12
Summary
Vericiguat’s efficacy and safety support its use as a suitable add-on therapy to address residual risk in HFrEF, particularly in patients with renal impairment, which limits GDMT implementation or intensification. In our patient with HFrEF and advanced CKD, in whom further GDMT escalation was precluded, vericiguat was well tolerated and associated with symptomatic and echocardiographic improvements.
References:
- Eur J Heart Fail 2021;23:1322-1324.
- Eur J Heart Fail 2021;23:1313-1321.
- Lancet 2022;400:1938-1952.
- Eur Heart J 2024;45:ehae666.1050.
- Circulation 2022;145:693-712.
- Front Cardiovasc Med 2025;12:1628411.
- Eur Heart J 2025;46:4583-4593.
- N Engl J Med 2023;388:117-127.
- Clin Transl Sci 2023;16:2458-2466.
- N Engl J Med 2020;382:1883-1893.
- J Assoc Physicians India 2024;72:63-68.
- Eur Heart J 2024;45.
This special report is supported by an education grant from the industry. 

