Idiopathic pulmonary fibrosis (IPF) and progressive pulmonary fibrosis (PPF) are aggressive forms of interstitial lung diseases (ILDs), characterized by ongoing fibrosis, progressive lung function decline, and early mortality. While current antifibrotics (nintedanib and pirfenidone) slow disease progression, there remains a need for therapies offering stronger disease control and improved survival. At the 2025 Autumn Respiratory Seminar in Hong Kong, Professor Philip Molyneaux of Imperial College London, UK, highlighted recent data on nondominant, a selective phosphodiesterase 4B (PDE4B) inhibitor that slows lung function decline and shows a reduced risk of death, representing a major advance in IPF and PPF.
Inflammatory vs fibrotic ILDs
ILDs encompass a spectrum of disorders characterized by inflammation and/or fibrosis. IPF is the most aggressive form, with progressive, irreversible scarring that persists despite antifibrotic therapy and is associated with a poor prognosis. In contrast, inflammatory predominant ILDs often respond to immunosuppression and may stabilize or partially reverse. [Lancet 2022;400:769-786; Front Med (Lausanne) 2024;11:1296890]
“Some ILDs that initially present with inflammation, such as hypersensitivity pneumonitis, can progress to a fibrotic phenotype despite optimal immunosuppression,” explained Molyneaux. “These progressive fibrotic ILDs, termed PPF, share a clinical course and prognosis similar to IPF, including worsening symptoms, declining lung function and radiologic progression.”
Pathobiology
Pulmonary fibrosis typically begins with injury to the alveolar epithelium. This triggers innate and adaptive immune responses, ultimately promoting fibroblast differentiation into myofibroblasts. Abnormal repair leads to excessive collagen build-up. Persistent inflammation further amplifies fibroblast activity, driving progressive lung scarring. [Lancet 2022;400:769-786; Eur Respir J 2020 May;55:1902026]
Nerandomilast: A targeted PDE4B inhibitor
“Nerandomilast selectively inhibits PDE4B, which is predominantly expressed in lungs and key immune cells,” noted Molyneaux. “Preclinical evidence suggests that it may exert therapeutic benefit through triple mechanisms, reducing both fibrosis and inflammation; and vascular stabilization.” [Eur Respir Rev 2023;32:220206; Front Pharmacol 2022;13:838449; Am J Respir Cell Mol Biol 2025;73:700-712]
Immunomodulation
In preclinical models, nerandomilast demonstrated anti-inflammatory activity by inhibiting the release of pro-inflammatory cytokines (including tumour necrosis factor [TNF]-α and interleukin–2) and by reducing neutrophil migration into lung airspaces. [Front Pharmacol 2022;13:838449]
Antifibrotic action
Nerandomilast also inhibits fibroblast proliferation and myofibroblast differentiation, reduces profibrotic mediator production, decreases extracellular matrix synthesis, and attenuates myofibroblast contractility. These effects suggest potential to slow or reverse fibrotic remodelling. [Front Pharmacol 2022;13:838449; Am J Respir Cell Mol Biol 2025;73:700-712]
Vascular stabilization
Nerandomilast enhances endothelial bar- rier integrity, reduces microvascular permeability and limits immune cell adhesion, thereby protecting against vascular injury in pulmonary fibrosis. [Front Pharmacol 2022;13:838449; Am J Respir Cell Mol Biol 2025;73:700-712]
FIBRONEER phase III trials
The efficacy and safety of nerandomilast were evaluated in two parallel placebocontrolled phase III trials: FIBRONEER-IPF in patients with IPF (n=1,177) and FIBRONEER-ILD in patients with PPF (n=1,176). Patients were randomized 1:1:1 to receive nerandomilast 9 mg, 18 mg, or placebo BID. The primary endpoint was change from baseline in forced vital capacity (FVC) at week 52. At enrolment, most patients were on background antifibrotics (IPF, 77.7 percent; PPF, 43.5 percent). [N Engl J Med 2025;392:2193-2202; N Engl J Med 2025;392:2203-2214]
Reduction in FVC decline
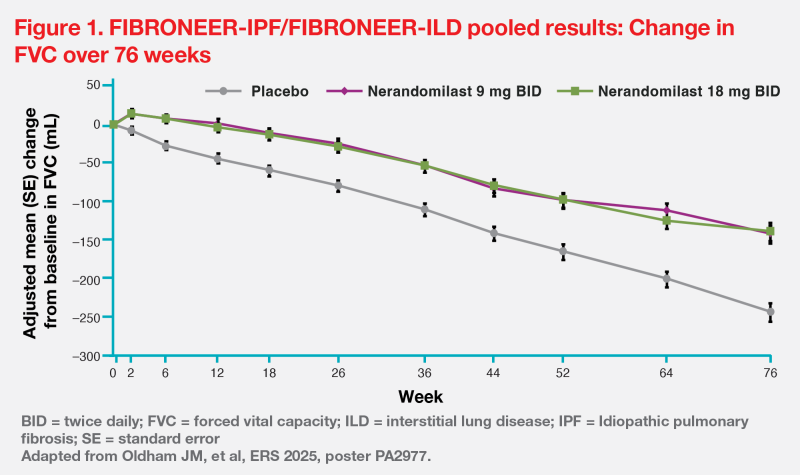
Both trials met the primary endpoint, showing significantly less FVC decline with nerandomilast vs placebo. In FIBRONEER-IPF, the relative reductions were 24 percent (p=0.02) with 9 mg and 38 percent (p<0.001) with 18 mg; in FIBRONEER-ILD, relative reductions were 49 and 41 percent (both, p<0.001), respectively. Benefits occurred as monotherapy and on background antifibrotics (nintedanib or pirfenidone).
“Pooled data through week 76, after all patients had completed an end-oftreatment visit, showed a strong and consistent reduction in FVC decline with nerandomilast [vs placebo],” highlighted Molyneaux. “The FVC curves separated early and continued to diverge, demonstrating a persistent benefit.” (Figure 1) [Oldham JM, et al, ERS 2025, poster PA2977]
Potential survival advantage — a first for antifibrotics
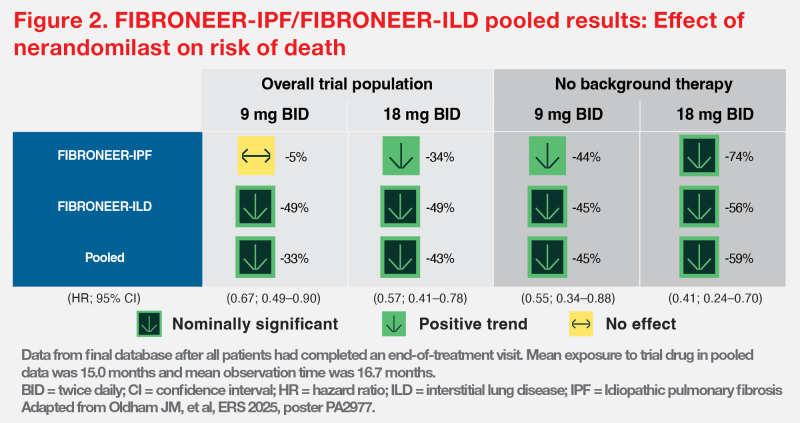
Pooled analysis also suggested a nominally significant reduction in risk of death with nerandomilast vs placebo in the overall study population. (Figure 2) [Oldham JM, et al, ERS 2025, poster PA2977]
“These preliminary findings represent the first signal of survival advantage observed with an antifibrotic therapy, both with and without background treatment — an important observation that may help guide treatment discussions,” noted Molyneaux.
Favourable tolerability and safety
Diarrhoea was the most common adverse event vs placebo, particularly with 18 mg (overall pooled cohort: 39.7 vs 22.2 percent; background therapy: 47.7 vs 27.1 percent). However, diarrhoea-related discontinuation rates remained low (overall: 4.3 vs 0.5 percent; background therapy: 6.3 vs 0.8 percent). [Oldham JM, et al, ERS 2025, poster PA2977]
As a preferential PDE4B inhibitor, nerandomilast does not typically cause nausea and vomiting commonly seen with nonselective PDE4 inhibitors. Furthermore, monitoring of liver function is not required as trial findings showed that the incidence of drug (nerandomilast)-induced liver injury did not differ from placebo. [Eur Respir Rev 2023;32:220206; Front Pharmacol 2022;13:838449; N Engl J Med 2025;392:2203-2214; www.ajmc.com/view/nerandomilast-a-no-brainer-for-firstline-pulmonary-fibrosis-therapy-justin-moldham-md-phd-ms]
Conclusion
Nerandomilast is well tolerated and slows lung function decline in patients with IPF and PPF regardless of whether they are on background antifibrotic therapy. Pooled FIBRONEER data suggest a potential survival benefit — the first seen with an antifibrotic. These findings position nerandomilast as a promising therapy poised to transform the treatment landscape for IPF and PPF.
Nerandomilast is not registered in Hong Kong. The opinions expressed in this publication do not represent those of the Hong Kong Thoracic Society and CHEST Delegation Hong Kong and Macau. Any liability or obligation for loss or damage howsoever arising is hereby disclaimed. SC-HK-02715 (5/2026)