History, investigation and initial treatments
This is a case of a 64-year-old woman with pulmonary arterial hypertension (PAH) poorly controlled on dual therapy, who was intolerant of selexipag and unsuitable for lung transplantation.
In 2018, the patient was initially diagnosed with anti-synthetase syndrome. At that time, she was managed and monitored at another hospital. Echocardiography showed a progressive increase in right ventricular systolic pressure (RVSP), rising from 55 mm Hg in 2023 to 64 mm Hg in 2024 and 84 mm Hg in July 2024. The patient was started on sildenafil 20 mg TID in August 2024.
In November 2024, upon referral to and presentation at our centre, the patient was grossly congested, in WHO functional class (FC) IV, and on long-term oxygen therapy (LTOT) at 1–2 L/min. Her N-terminal pro-B-type natriuretic peptide (NT-proBNP) level was elevated at 6,076 pg/mL. (Table) She was admitted shortly for diuresis and treatment optimization. The transplant team evaluated the patient and determined that she was not a candidate due to frailty and relatively advanced age.
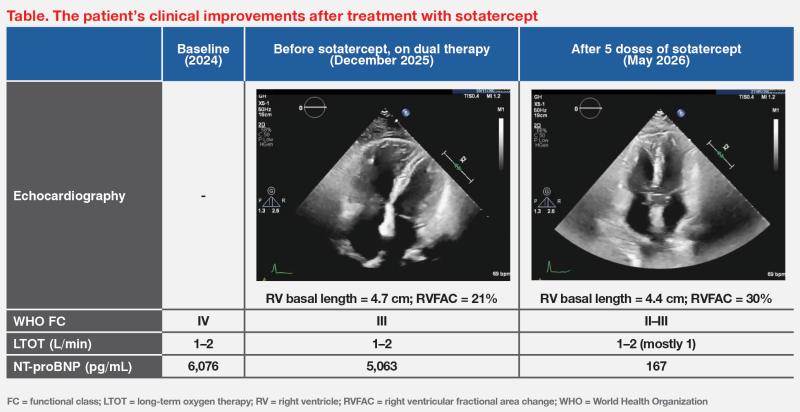
After stabilization, the patient was started on macitentan 10 mg QD in June 2025. Right heart catheterization (RHC) in August 2025 showed right atrial pressure of 4 mm Hg, pulmonary capillary wedge pressure of 5 mm Hg, markedly elevated mean pulmonary artery pressure (mPAP) of 41 mm Hg, and pulmonary vascular resistance (PVR) of 10 WU. Cardiac output and cardiac index were mildly reduced at 3.57 L/min and 2.26 L/min/m2, respectively. Despite dual therapy, the RHC findings were still alarming and the patient’s WHO FC was III. We discussed the next steps in management with the patient.
Between November and December 2025, the patient was briefly treated with selexipag, but could not tolerate it due to generalized discomfort, headache, diarrhoea, and muscle pain. At the same time, her NT‑proBNP level was elevated at 5,063 pg/mL, which could partly be due to a concomitant chest infection.
Treatment with sotatercept
In early 2026, after treatment of chest infection, the patient was started on subcutaneous sotatercept 0.3 mcg/kg Q3W, which was subsequently uptitrated to 0.7 mcg/kg Q3W.
After five doses of sotatercept, the patient reported subjective improvement. NT proBNP decreased markedly to 167 pg/mL, and WHO FC improved to II–III. LTOT remained as 1–2 L/min, but the patient predominantly required 1 L/min. (Table)
The patient tolerated sotatercept well and reported no adverse events (AEs). Platelet counts remained within the normal range throughout treatment. Haemoglobin (Hb) was mildly elevated (14.1–15.9 g/dL) but still within normal range.
Last seen in late May 2026, the patient remained clinically stable on triple therapy with sotatercept, macitentan and sildenafil. She has not been hospitalized since initiating sotatercept.
Discussion
PAH is a rare disease that is difficult to diagnose, with a diagnostic delay of ≥2 years. Consequently, patients frequently present at an advanced stage, as demonstrated in our case.1
How does sotatercept address unmet needs?
Modern PAH therapies, such as macitentan, sildenafil and selexipag, target the endothelin-1 (ET-1), nitric oxide (NO) and prostacyclin (PGI2) pathways.2 These agents have transformed PAH from a historically fatal disease with a median survival of 2.8 years to a condition with a 3-year survival rate of >70 percent.1,3
However, each drug class provides only temporary clinical stability, lasting several years. While successive use of drugs from different classes may extend the duration of clinical stability, we have observed initial signs of clinical deterioration in patients treated with triple therapy at our centre.
Sotatercept is the first activin signalling inhibitor approved for treatment of PAH. Acting on the fourth PAH pathway, the mechanism of action of sotatercept is fundamentally different from that of other modern PAH therapies, which mainly promote vasodilation. By restoring the balance between antiproliferative and proproliferative signalling pathways, sotatercept directly targets the molecular roots of PAH rather than just treating symptoms.2,4
STELLAR, a multicentre, double-blind, phase III trial, evaluated the efficacy and safety of sotatercept in 323 adult patients with PAH WHO FC II (48.6 percent) or III (51.4 percent) who were receiving stable background therapy (triple therapy, 61.3 percent; prostacyclin infusion therapy, 39.9 percent; dual therapy, 34.7 percent; monotherapy, 4.0 percent). Patients were randomized 1:1 to receive subcutaneous sotatercept or placebo Q3W.5
Sotatercept was associated with a significant improvement in 6- minute walk distance (6MWD) at week 24 (primary endpoint) vs placebo (difference, +40.8 m; p<0.001). Of note, more patients on sotatercept vs placebo experienced improvement in WHO FC at week 24 (29.4 vs 13.8 percent; p<0.001). In terms of quality of life (QoL), both PAH-SYMPACT Physical Impacts and Cardiopulmonary Symptoms domain scores were improved with sotatercept vs placebo.5
Although 6MWD could not be measured in our patient, subjective improvement in symptom control was reported. After sotatercept treatment, her WHO FC improved from III to II–III. LTOT remained as 1–2 L/min, but she predominantly required 1 L/min. (Table)
NT-proBNP is one of the important markers for risk stratification and clinical monitoring in PAH. A level <300 pg/ mL effectively indicates low risk, while a level >1,100 pg/mL indicates high risk.6 In STELLAR, sotatercept also significantly improved NT-proBNP levels vs placebo (difference, -441.6 pg/ mL; p<0.001).5 Consistent with these findings, our patient’s NT-proBNP level decreased from 5,063 (high-risk level) to 167 pg/mL (low-risk level) after five doses of sotatercept.
After a median of 32.7 weeks in STELLAR, treatment with sotatercept resulted in an 84 percent lower risk of a composite of all-cause death or nonfatal clinical worsening event vs placebo (hazard ratio [HR], 0.16; 95 percent confidence interval [CI], 0.08–0.35; p<0.001).5
Sotatercept is well-tolerated, with a reported discontinuation rate due to AEs of only 1.8 percent (vs 6.2 percent with placebo). Additionally, rates of overall AEs (84.7 vs 87.5 percent), severe AEs (8.0 vs 13.1 percent) and serious AEs (14.1 vs 22.5 percent) at week 24 were all numerically lower with sotatercept vs placebo. AEs that occurred more frequently with sotatercept than placebo included epistaxis (12.3 vs 1.9 percent), dizziness (10.4 vs 1.9 percent), telangiectasia (10.4 vs 3.1 percent), thrombocytopenia (6.1 vs 2.5 percent), increased Hb levels (5.5 vs 0 percent), and increased blood pressure (3.7 vs 0.6 percent).5 Our patient had a slight rise in Hb level that remained within the normal range and did not require treatment. Regular monitoring of Hb and platelet levels before each dose of sotatercept for at least the first five doses is suggested.4
SOTERIA: Long-term study of sotatercept
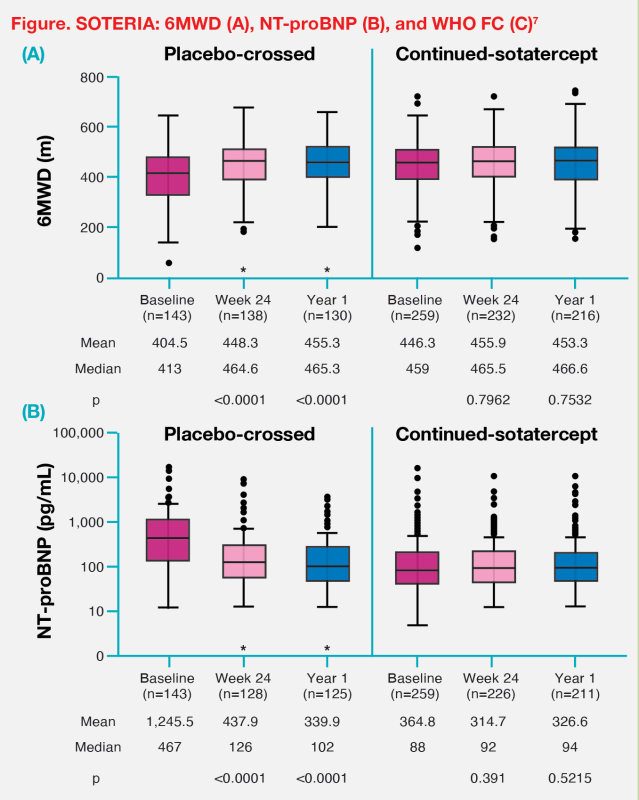
SOTERIA is an ongoing open-label study assessing the long-term safety and efficacy of sotatercept in 426 patients with PAH: 143 rolled over from a prior study’s placebo arm (placebo-crossed group), 259 continued from a prior study’s sotatercept arm (continued-sotatercept group), and 24 were transferred from a blinded treatment arm of ZENITH or HYPERION. Mean follow-up was 448.6 days.7
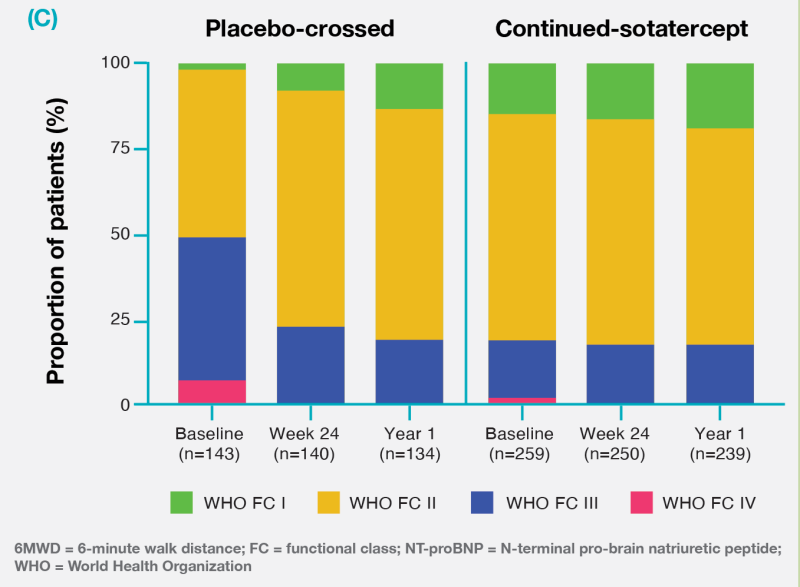
In SOTERIA, the placebo-crossed group showed significant improvements in 6MWD and NT-proBNP at week 24, which were largely sustained at year 1 (p<0.0001 for both timepoints). By year 1, 6MWD and NT-proBNP in the placebo-crossed group were comparable to those in the continued-sotatercept group. (Figure) The proportion of placebo-crossed patients in WHO FC I or II rose from 51.0 percent at baseline to 77.1 percent at week 24 and 79.9 percent at year 1, reflecting improved WHO FC over time.7 (Figure)
In the continued-sotatercept group, 6MWD, NT-proBNP, and the proportions of patients in WHO FC I or II at baseline in SOTERIA were similar at week 24 and year 1, indicating durable clinical efficacy through 1 year.7 (Figure)
Conclusion
Add-on sotatercept has a favourable safety profile and potential disease-modifying properties and represents an effective strategy to improve patients’ exercise capacity, WHO FC and NT-proBNP, and delay clinical worsening. Clinically, I would favour using sotatercept in PAH patients who remain at intermediate or high risk despite triple therapy, as they are likely to derive the greatest benefit. Another suitable group would be those on dual therapy who cannot tolerate a third agent, like our patient.
References:
- Eur Respir Rev 2007:102:8-12.
- Int J Cardiol Congenit Heart Dis 2025:21:100594.
- Rev Port Pneumol (2006) 2017;23:124-131.
- Winrevair Hong Kong Prescribing Information, March 2025.
- N Engl J Med 2023;388:1478-1490.
- www.pahriskcalculatorlt.com/?utm_medium=referral&utm_source=pahinitiative.com
- Eur Respir J 2025;66:2401435.
This special report is supported by an education grant from the industry