
Laboratory Tests and Ancillaries
Serum testosterone levels should be obtained between 07:00-11:00 am. Total testosterone level should be compared with the normal ranges established by each laboratory.
Testosterone Serum Level
 Hypogonadism in Males - Late-Onset_Diagnostics 1
Hypogonadism in Males - Late-Onset_Diagnostics 1
Normal Serum Testosterone
There are no specific lower limits of normal serum testosterone in older men. It is generally agreed that a total testosterone level >12 nmol/L (>345 ng/dL) does not require testosterone substitution.
Low Level
Based on measurements taken in younger men, if total testosterone level is <8 nmol/L (<231 ng/dL), then testosterone substitution should be considered.
Low-Low/Normal Level
In patients with the following, testosterone substitution may be considered: A total testosterone level between 8-12 nmol/L (231-345 ng/dL) AND the presence of symptoms (please see Clinical Presentation section) that are not due to other causes.
Repeat Testosterone Serum Level and Measure Follicle-stimulating Hormone (FSH) and Luteinizing Hormone (LH) Levels
If the testosterone level is low or at the lower limit of normal, the level should be repeated for confirmation. Follicle-stimulating hormone and luteinizing hormone levels should also be measured.
 Hypogonadism in Males - Late-Onset_Diagnostics 2
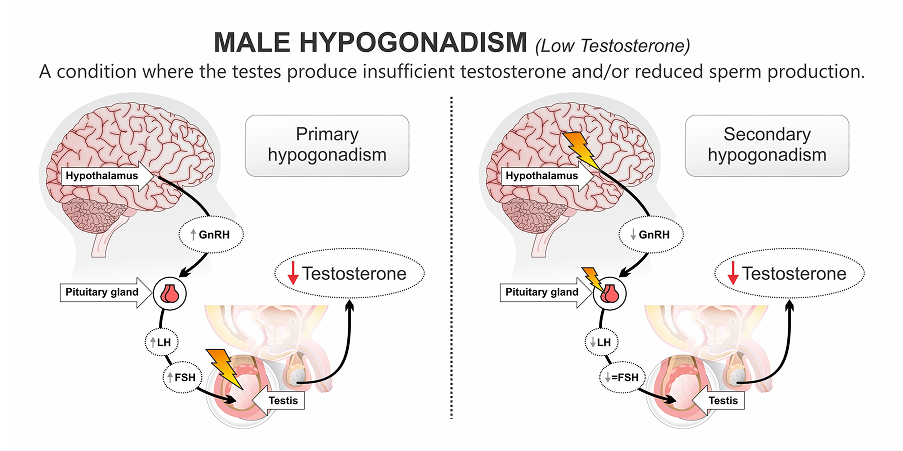
Hypogonadism in Males - Late-Onset_Diagnostics 2Primary Hypogonadism (Testicular Origin)
A low testosterone level with increased FSH and LH suggests a testicular failure origin for hypogonadism.
Secondary Hypogonadism (Hypothalamic-Pituitary Origin)
Low testosterone level with decreased FSH and LH is suggestive of a hypothalamic-pituitary origin of disease. Further endocrinological work-up may be needed.
Other Investigations
Measure complete blood count, urinalysis, and blood chemistry parameters. Lipid profile and liver function tests are also recommended to assess the patient’s risk status. Measure prolactin levels if low sexual desire (or other indicative signs or symptoms) and secondary hypogonadism are present.
Imaging
A pituitary magnetic resonance imaging (MRI) is suggested in secondary severe hypogonadism (<6 nmol/L) and in secondary hypogonadism with elevated prolactin levels, symptoms specific to a pituitary mass, and/or the presence of anterior pituitary hormone deficiency.