
Clinical Presentation
Tinea Corporis (Ringworm)
 Tinea Corporis, Cruris and Pedis_Initial Assesment 1
Tinea Corporis, Cruris and Pedis_Initial Assesment 1
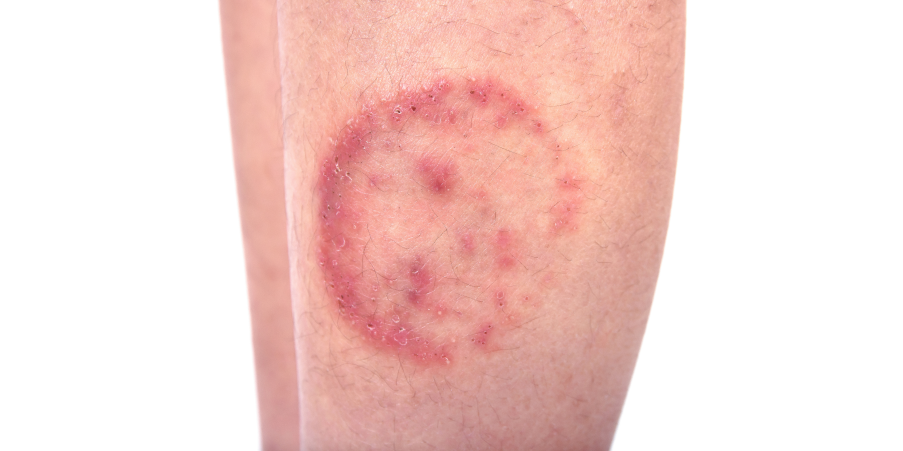
The patient usually presents with lesions of varying size, degree of inflammation, and depth of involvement found on the trunk, extremities, or face, excluding the beard area in men. Lesions are characterized as single or multiple, round or oval, and scaly and have central clearing and elevated reddened edges. Lesions have sharp, serpiginous, annular, and very irregular borders with a polycyclic pattern. Papules or pustules may be present on the border. Pruritus may or may not be present.
Tinea Cruris (Jock Itch)
 Tinea Corporis, Cruris and Pedis_Initial Assesment 2
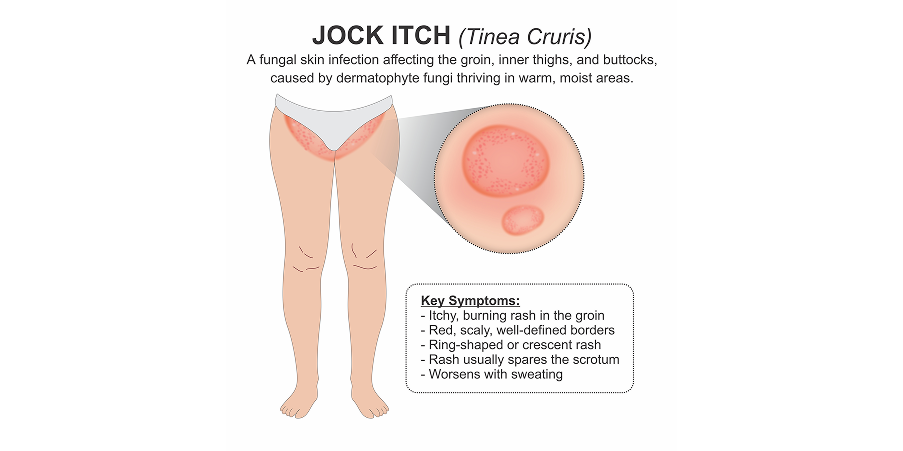
Tinea Corporis, Cruris and Pedis_Initial Assesment 2Lesions are found on the groin and may affect the proximal medial thighs and extend to the buttocks and abdomen. Scrotum and penis tend to be unaffected. Tinea cruris is more common in men than women with risk factors, including obesity and immunodeficiency. Red scaling lesions with raised borders have pustules and vesicles at the active edge of the infected area. Maceration is usually present. Patients usually complain about burning and itching. Feet may also be affected and become the source of the infection, as tinea pedis and tinea cruris have the same causative agents. Recurrent tinea cruris may be prevented by treating the concomitant tinea pedis infection and other dermatophyte infections.
Tinea Pedis (Athlete’s Foot)
 Tinea Corporis, Cruris and Pedis_Initial Assesment 3
Tinea Corporis, Cruris and Pedis_Initial Assesment 3Interdigital Type
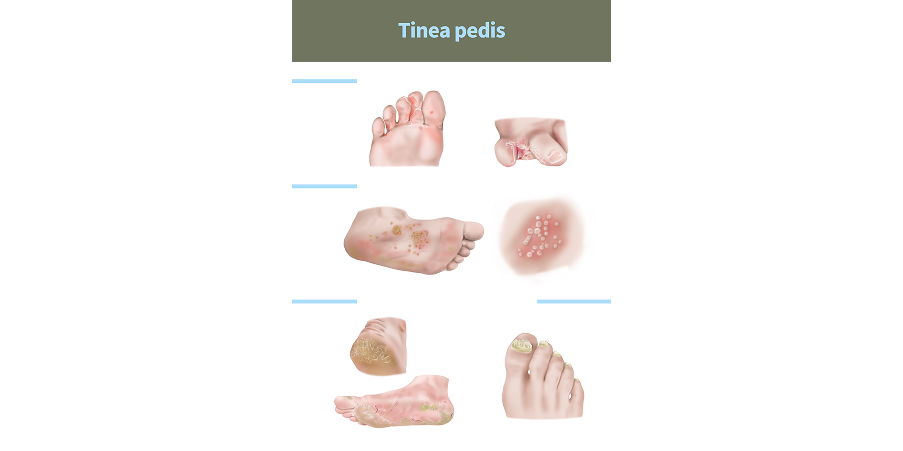
Interdigital type is the most common form of tinea pedis. Maceration, fissuring, and scaling of the interdigital spaces of the fourth and fifth toes are noted. The patient usually complains of itching or burning that is most intense when shoes and socks are removed. Secondary infection with Gram-positive and Gram-negative bacteria can result in foul odor, maceration, erosions, and crusting, which is referred to as the dermatophytosis complex.
Plantar Hyperkeratotic or Moccasin Type
The sole of the foot is typically covered with a fine silvery scale. The skin is pink, tender, and pruritic. Erythema is more prominent on the distal dorsum of the foot. Disease takes a chronic course and is resistant to treatment.
Vesicular or Vesiculobullous Type
The vesicular or vesiculobullous type is the least common form, primarily on the sides of the feet. This may mimic acute contact dermatitis, but the latter does not affect intertriginous areas. This presents with intensely pruritic vesicles, which may also be painful. Vesicles may coalesce to form a bulla. Lesions develop more rapidly than other forms of tinea pedis.
History
Dermatophytoses are most often diagnosed through a careful clinical history and a comprehensive physical examination. Important history includes the patient’s immune status, comorbidities, residence and travel history, recent trauma or surgery, prior antimicrobial use, hospitalizations, lifestyle, sexual activity, incarceration history, close contact with infected individuals, and animal exposure or bites.
 Tinea Corporis, Cruris and Pedis_Initial Assesment 4
Tinea Corporis, Cruris and Pedis_Initial Assesment 4
Physical Examination
Evaluating the appearance, location, and progression of skin lesions helps identify the possible causative agent.