
Introduction
 Tinea Unguium_Disease Background 1
Tinea Unguium_Disease Background 1Tinea unguium is a specific onychomycosis (fungal infection of the nailbed, nail plate, or both) caused by dermatophytes. This is also called dermatophytic onychomycosis and more commonly affects the toenails than the fingernails.
Epidemiology
Tinea unguium is a common fungal nail infection that accounts for about 15% of all nail disorders, while fungal nail infections comprise approximately 10% of all dermatophytosis cases. This is more common in men than in women. Tinea unguium is most seen in adults, however, the superficial variant of tinea unguium is more commonly seen in children than in adults.
Dermatophytes are the primary cause of most onychomycosis cases in Western countries and are responsible for about 40–68% of cases in Southern Europe and 40–48% of cases in Asian and Middle Eastern countries. The high prevalence of tinea unguium in North America has been partly attributed to the migration and spread of dermatophytes from regions such as West Africa and Southeast Asia. Onychomycosis are the most prevalent forms of dermatophytosis in Europe.
Etiology
 Tinea Unguium_Disease Background 2
Tinea Unguium_Disease Background 2Tinea unguium is most commonly caused by Trichophyton rubrum. This may also be caused by yeasts and non-dermatophyte molds.
Pathophysiology
Tinea unguium is acquired through direct contact of the nail with dermatophytes, yeasts, or non-dermatophyte molds in the environment. This may also be acquired from a pre-existing fungal infection from surrounding skin (eg tinea pedis). There is dermatophyte production of keratinases that facilitates invasion, infecting the nail bed. This eventually infects the viable nail matrix, leading to the nail bed becoming hyperkeratotic and thickened to shed the fungal infection. Invasion of the overlying nail plate leads to detachment and distortion.
Risk Factors
Risk factors for tinea unguium are aging, male gender, peripheral vascular diseases, diabetes mellitus (DM), occlusive footwear, human immunodeficiency virus (HIV), presence of tinea pedis, immunosuppression, atopy, hyperhidrosis, exposure to individuals with tinea pedis or onychomycosis, psoriasis, trauma, poor nail grooming, and smoking.
Classification
Clinical Subtypes
 Tinea Unguium_Disease Background 3
Tinea Unguium_Disease Background 3
Onychomycosis is classified based on the route of infection and clinical presentation.
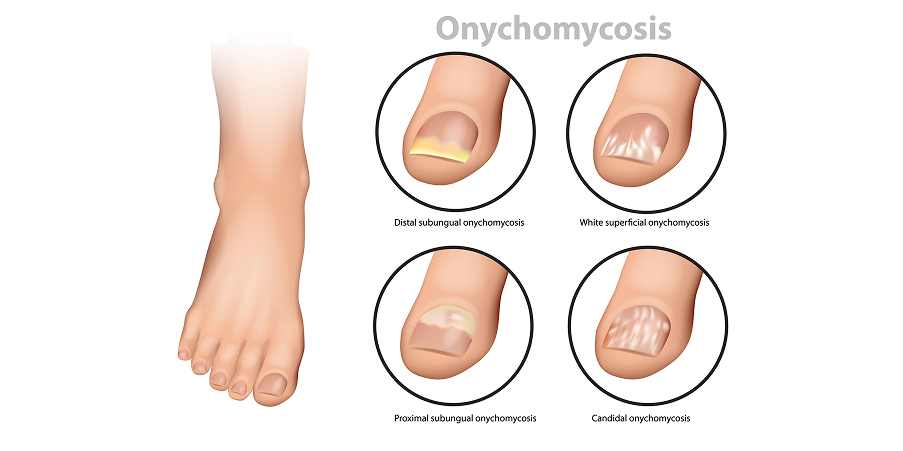
Distal Lateral Subungual Onychomycosis (DLSO)
Distal lateral subungual onychomycosis is the most common type of onychomycosis and involves 90% of infections. Invasion occurs in the distal subungual space and at the distal lateral groove. This more commonly involves the toenails. The nail plate looks opacified and hyperkeratotic; its distal portion may break away. The nail’s discoloration results from keratinous debris accumulating between the nail plate and the nail bed. Subungual hyperkeratosis and onycholysis (separation of the nail plate from the nail bed) are frequent findings. Splinter hemorrhages are seen secondary to mild inflammation compressing small blood vessels. The most common cause is Trichophyton rubrum. This may also be caused by Trichophyton tonsurans, Trichophyton mentagrophytes, and Epidermophyton floccosum.
Superficial White Onychomycosis (SWO)
Superficial white onychomycosis is the second most prevalent type of onychomycosis and involves 10% of infections. The dorsal surface of the nail plate is invaded. There is minimal inflammation, and the nail becomes soft and crumbly with a white-colored rough surface. The nail plate is not thickened and remains attached to the nail bed. This is marked by dull, white patches appearing on the nail surface. This is typically caused by Trichophyton mentagrophytes but may also be caused by non-dermatophyte molds.
Proximal Subungual Onychomycosis
Proximal subungual onychomycosis is the least common form of onychomycosis in healthy individuals and may be an early indicator of HIV infection. The toenails are more commonly infected than fingernails. Infection enters at the cuticle, and the proximal nail bed is always involved. This spreads distally, so if left untreated, the entire nail plate will be affected. The nail plate is typically white in color. Subungual hyperkeratosis and proximal onychomycosis are usually present. This is usually caused by T rubrum but can be caused by Trichophyton megnini, T tonsurans and T mentagrophytes.
Endonyx Onychomycosis
Endonyx onychomycosis affects only the inner portion of the nail plate while leaving the nail bed uninvolved. Typical features include nail discoloration and splitting, with subungual hyperkeratosis notably absent. Trichophyton soudanense is the organism most strongly linked to endonyx onychomycosis, though other species such as Trichophyton violaceum can produce the same pattern.
Candidal Onychomycosis
Candidal onychomycosis is commonly found in patients diagnosed with chronic mucocutaneous candidiasis. This more commonly affects fingernails. Candida invades the nail bed or plate directly or may indirectly involve the nail through infecting the nail bed, folds, or hyponychium. The entire nail thickens and turns yellow-brown; progression may lead to total dystrophy of the nails. This is usually caused by Candida albicans or other Candida sp. This may have some resistance to oral antifungal agents.
Total Dystrophic Onychomycosis
Total dystrophic onychomycosis is the most advanced form of onychomycosis. The nail plate is almost completely destroyed, which leads to a thickened, ridged nail bed covered with keratotic debris. This may be the end result of the above four forms.
Mixed Pattern Onychomycosis
Mixed pattern onychomycosis is defined by the coexistence of ≥1 of the previously described subtypes. These are the most frequent mixed forms, combining superficial white onychomycosis with either distal lateral subungual or proximal subungual onychomycosis.