
Introduction
 Neuropathic Pain_Disease Background 1
Neuropathic Pain_Disease Background 1Neuropathic pain arises as a consequence of a lesion or disease affecting the somatosensory pathway of the peripheral and/or central nervous system (CNS). This is described as pain that is burning, stabbing, shooting, electrical-like, or mimicking pins and needles or insects crawling, which may be constant or paroxysmal. Nerve conduction blockage causes nerve dysfunction, leading to numbness, weakness, and loss of deep tendon reflexes in the area of the involved nerve. Neuropathic conditions (eg brain infarction, spinal cord trauma, ischemic neuropathies) also cause aberrant symptoms of spontaneous and provoked pain.
Epidemiology
The prevalence of neuropathic pain varies due to its multiple etiologies and presentations. In Malaysia, the prevalence of neuropathic pain is estimated to range from 1.5% of the general population. In the Philippines, previous and recent studies showed prevalence rates of 42% and 58%, respectively. In a study from Indonesia, 54% of 110 patients with type 2 diabetes mellitus and neuropathy had painful diabetic neuropathy. In Europe, it is estimated to afflict 7-8% of the general population. In studies using population-based questionnaires in Canada, it shows the prevalence as 4-8%. Diabetic polyneuropathy has been estimated to occur in 10-100% of diabetic patients in the Western world.
Overall, neuropathic pain occurs more frequently in women than in men and is more common in individuals older than 50 years old. However, its prevalence varies depending on the underlying cause. Postherpetic neuralgia affects nearly all cases and is most common among the elderly. In patients with AIDS, about 30% experience neuropathic pain. Among individuals with diabetes mellitus, 20-24% are affected, with higher prevalence in those with longer disease duration. Additionally, chemotherapy-induced neuropathy affects around 20-50% of patients with cancer.
Etiology
Neuropathic pain can result from several conditions, including metabolic disorders (eg diabetes mellitus, nutritional deficiencies), vascular conditions (eg stroke), inflammatory diseases (eg autoimmune diseases, multiple sclerosis), infiltrative diseases (eg amyloidosis), hematologic disorders (eg plasma cell disorders, polycythemia vera), infectious causes (eg post viral, syphilis), and neoplastic conditions. This can also be caused by certain drugs or toxins such as chemotherapeutic agents, and trauma (eg spinal cord injury), as well as genetic disorders.
Pathophysiology
Pathophysiological mechanisms involved in neuropathic pain include sensory nerve conduction blockage, which causes nerve dysfunction and leads to sensory impairment (e.g., numbness). If there are concomitant motor nerve involvement, weakness and loss of deep tendon reflexes may also be observed. Proliferation of sodium channels at the neuroma site and along the length of the peripheral nerve after injury can result in foci of ectopic activity, leading to spontaneous neuropathic pain. Sympathetic axons may sprout around the dorsal root ganglion, where neuropathic pain can be sympathetically mediated. There is also diminished inhibitory control over dorsal horn neurons through various mechanisms. Additionally, central sensitization of the dorsal horn neurons is manifested as a heightened response to noxious stimuli, as well as pain associated with stimuli within the non-noxious range.
Risk Factors
Several factors may predispose an individual to the development of neuropathic pain. These include age, particularly middle adulthood (50–64 years old), and gender, as chronic pain is more prevalent in women. The specific site of injury also plays a role, since mono- or polyneuropathies can occur in different anatomical locations. Sociodemographic factors may also influence risk. Neuropathic pain is linked to several behavioral and social factors, some of which are modifiable and therefore important targets for preventive strategies. For example, alcohol consumption and smoking have both been associated with an increased risk of neuropathic pain. Body mass index (BMI), body weight, and waist circumference have been shown to be associated with neuropathic pain among individuals with diabetes. In addition, genetic backgrounds may either increase susceptibility to or provide protection against neuropathic pain. Emotional and cognitive well-being can also affect how individuals perceive and respond to chronic pain.
Classification
Common Neuropathic Pain Syndromes
Central Neuropathic Pain
For central neuropathic pain, the pain may be burning, shooting, aching, or pricking and is often associated with dysesthesia, hyperalgesia, or allodynia to brush or cold. This is seen among patients with stroke, spinal cord injury (SCI), and multiple sclerosis.
Painful Diabetic Peripheral Neuropathy (DPN)
Diabetic peripheral neuropathy is symmetrical sensory loss and burning, shooting, stabbing, or severe deep aching pain of both upper and lower extremities among patients with diabetes mellitus (DM). This affects about 50% of patients with diabetes mellitus. Pain may be accompanied by allodynia and hyperalgesia. Symptoms may worsen at night.
Postherpetic Neuralgia (PHN)
 Neuropathic Pain_Disease Background 2
Neuropathic Pain_Disease Background 2Postherpetic neuralgia is pain persisting for >3 months after herpes zoster skin lesions have healed. Risk factors for developing postherpetic neuralgia include: All patients >50 years old with herpes zoster virus (HZV) infection; patients with a greater degree of skin surface area involved and more severe pain at presentation of HZV infection; patients with HZV ophthalmicus; patients who experience sensory dysfunction on the affected dermatome; and patients with painful prodrome prior to rash.
Patients at greatest risk for developing postherpetic neuralgia should be offered antiviral treatment. The diagnostic clinical features of postherpetic neuralgia are: Pain localized to the dermatome affected by the herpes zoster rash; pain may be described as burning, throbbing, sharp, or shooting; allodynia; pain accompanying movement; areas of scarring or hypopigmentation caused by herpes zoster rash; and the presence of psychosocial stress.
Trigeminal Neuralgia (TN)
 Neuropathic Pain_Disease Background 3
Neuropathic Pain_Disease Background 3Trigeminal neuralgia is characterized by intermittent unilateral facial pain following the unilateral sensory distribution of the trigeminal nerve, typically radiating to the maxillary or mandibular area. Ophthalmic division pain alone occurs in <5% of patients. Pain is quite severe, characterized as stabbing, or electric shock-like sensation. Pain may be brief and paroxysmal but may occur in multiple attacks several times a day, with no pain between episodes. Typically, with normal physical examination findings, although mild light touch or pin perception loss has been described in the central area of the face. The average age of pain onset in idiopathic TN is usually in the sixth decade of life, but this may occur at any age. Symptomatic or secondary TN tends to occur in younger patients. Common triggers precipitating pain attacks include light touch or vibration and activities such as shaving, face washing, or chewing.
Postsurgical Neuropathic Pain
Postsurgical neuropathic pain is a peri-incisional sensory loss, pain, and allodynia for >3 months after surgery such as phantom pain following amputation or mastectomy.
Human Immunodeficiency Virus (HIV)-Related Neuropathy
Human immunodeficiency virus-related neuropathy is a symmetrical painful paresthesia that is most prominent in the toes and soles of the feet among patients living with HIV.
Cervical and Lumbosacral Radiculopathy (Herniated Intervertebral Disc)
Cervical and lumbosacral radiculopathy is lancinating pain radiating into the anterior thigh (L2/3) or lower leg (L4-S1) with motor weakness or sensory loss. Motor and sensory impairments usually follow the corresponding myotome and dermatomes.
Please see Low Back Pain disease management chart for further information.
Complex Regional Pain Syndrome
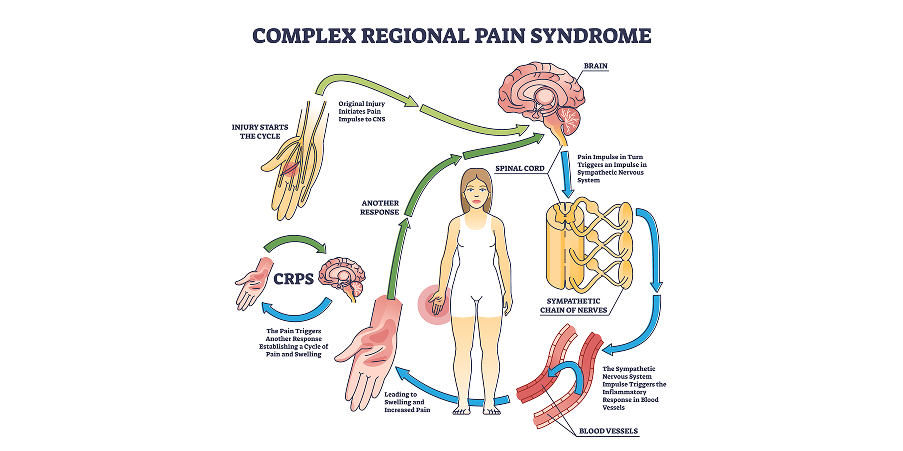 Neuropathic Pain_Disease Background 4
Neuropathic Pain_Disease Background 4Complex regional pain syndrome is a regional (eg limb) pain together with edema, cutaneous blood flow, and sweating abnormalities.