
Principles of Therapy
 Parkinsons Disease and Dementia_Management 1
Parkinsons Disease and Dementia_Management 1The choice of medication depends on the following factors: Stage of disease, relative effectiveness and adverse effect profile of the drugs, clinician experience, patient’s comorbidities, degree of functional disability, level of physical activity and productivity, employment status, and preference. Improvements in drug efficacy and symptom control may be measured in clinical trials using rating scales (eg Hoehn and Yahr scale, the Schwab and England scale, and the Unified Parkinson’s Disease Rating Scale).
Treatment Goals
The goals for treatment are to alleviate motor and nonmotor symptoms that interfere with the patient's daily activities; limit complications as the disease progresses; slow down or modify disease progression; motor symptoms are relieved by supplementation of cerebral dopamine; and nonmotor dysfunction is relieved by symptomatic treatment.
Pharmacological therapy
Dopamine Precursor
Levodopa
 Parkinsons Disease and Dementia_Management 2
Parkinsons Disease and Dementia_Management 2Levodopa remains the most effective treatment for Parkinson’s disease symptoms. This is the preferred initial therapy in Parkinson’s disease patients with cognitive impairment, with atypical presentation, or in the elderly. This is recommended as the initial therapy for patients with early Parkinson’s disease who seek treatment for motor symptoms. This should be initially prescribed as an immediate-release Levodopa and with the lowest effective dose to minimize adverse effects. Studies have shown that Levodopa demonstrates greater improvement in mobility compared to monoamine oxidase B (MAO-B) inhibitors and dopamine agonists (DA) when given early in the disease. This is more likely to induce dyskinesia compared to DA but the prevalence of severe or disabling dyskinesia is low within a 5-year period.
Levodopa acts as a dopamine precursor that is converted into dopamine in the brain. Levodopa rapidly decarboxylates peripherally so that little unchanged drug is available to cross the blood-brain barrier. Always administer in combination with a peripheral dopa-decarboxylase inhibitor (Carbidopa) to increase the amount of Levodopa entering the brain. Therefore, less Levodopa needs to be administered, ensuring a more rapid response to therapy and less peripheral side effects. This reduces debilitating symptoms and is most effective in alleviating bradykinesia and rigidity. Incidence of dyskinesia and “on-off” fluctuation with long-term use is common. Behavioral disturbances (eg hypersexuality, excessive gambling and shopping, and compulsive eating) have occurred with long-term use.
Dopamine Agonists (DA)
Examples of ergot-derived drugs: Bromocriptine, Cabergoline, Lisuride, Pergolide
Examples of non-ergot derived drugs: Apomorphine, Piribedil, Pramipexole, Ropinirole, Rotigotine
Dopamine agonists are recommended as monotherapy or as an adjunctive therapy to Levodopa. These are effective in the treatment of patients with early Parkinson’s disease and motor symptoms. One may prescribe DA as the initial treatment in early Parkinson’s disease patients <60 years who are at higher risk of developing dyskinesia. These should be prescribed at the lowest effective dose possible to provide therapeutic benefit. Systematic screening of patients for risk factors for adverse effects associated with medication use or disease progression are done by administering questionnaires (eg the Questionnaire for Impulsive-Compulsive Disorders in Parkinson’s Disease [QUIP], Epworth Sleepiness Scale [ESS]).
Dopamine agonists are not recommended for patients with early Parkinson’s disease who are at higher risk of medication-related adverse effects, >70 years old, have a history of impulse control disorders and preexisting cognitive impairment, or have excessive daytime sleepiness or hallucinations. When DA treatment is to be discontinued due to adverse effects, it is recommended to monitor for symptoms of dopamine agonist withdrawal syndrome (DAWS) and to gradually decrease the dosage to minimize symptoms. These act to stimulate dopamine receptors.
Dopamine agonists are less likely to have motor fluctuations in later stages of the disease when therapy is started in early disease. These are less effective than Levodopa in controlling rigidity and bradykinesia but less likely to cause dyskinesia. Piribedil, Pramipexole and Ropinirole do not stimulate serotonin receptors, thus cause less side effects than other dopamine agonists. Apomorphine is used to stabilize patients experiencing refractory motor fluctuations, but subcutaneous injection is suitable for capable and motivated patients only. Bromocriptine may be used in early and late disease. Cabergoline is found to be clinically useful in preventing or delaying the onset of motor fluctuations. Pergolide is useful for initial therapy of Parkinson’s disease. Pramipexole is an effective treatment of motor complications in preventing or delaying motor symptoms and delaying dyskinesia. Ropinirole may be considered in early Parkinson’s disease, in patients who develop motor fluctuations, and for delaying dyskinesia. Rotigotine may be used in idiopathic Parkinson’s disease as monotherapy or in combination with Levodopa. Behavioral disturbances (eg hypersexuality, excessive gambling and shopping, and compulsive eating) have occurred with long-term use. Dopamine agonists have antioxidant effects, but a neuroprotective benefit has yet to be proven.
Monoamine Oxidase B Inhibitors
Example drugs: Rasagiline, Safinamide, Selegiline
Selegiline in early Parkinson’s disease was shown to postpone the need for dopaminergic treatment by several months. Monoamine oxidase B inhibitors are associated with mild to moderate benefits in symptomatic control of Parkinson’s disease. These are recommended as monotherapy or as an adjunct to Levodopa and may be associated with a higher risk of discontinuation due to adverse effects. For patients with motor fluctuations, Rasagiline is recommended to reduce off time. This may be used initially for mild symptomatic benefit prior to the start of dopaminergic therapy. Neuroprotective benefit has yet to be proven.
Monoamine oxidase B inhibitors act to inhibit the activity of the enzyme monoamine oxidase B irreversibly, preventing the metabolism of naturally occurring dopamine and dopamine formed from Levodopa. The action of Levodopa is prolonged by the addition of Selegiline; therefore, Levodopa’s “wearing off” fluctuations are decreased. These may provide slight improvement in symptoms. Safinamide has been approved by the United States Food and Drug Administration (US FDA) as an add-on treatment to Levodopa or Carbidopa in patients with Parkinson’s disease having off time.
Catechol-O-Methyltransferase (COMT) Inhibitors
Example drugs: Entacapone, Opicapone and Tolcapone
Catechol-O-Methyltransferase (COMT) inhibitors are recommended as adjuncts to Levodopa and Carbidopa drug combination. For patients with motor fluctuations, Entacapone is recommended to reduce off time. Tolcapone has limited use due to the risk of hepatotoxicity and may be used only when other adjunctive treatments fail. This is a selective, potent, peripheral, and, to a lesser extent, central reversible inhibitor of catechol-O-methyltransferase, which prevents the metabolism of naturally occurring dopamine and dopamine formed from Levodopa. Hence, more Levodopa reaches the central nervous system and is converted to dopamine. This may decrease motor fluctuations when administered as adjuncts to Levodopa. A lower effective dose of Levodopa is required, thus reducing side effects. Trials have shown that COMT inhibitors do not have an effect on delaying motor complications.
Anticholinergics
Example drugs: Benztropine, Benzhexol (Trihexyphenidyl), Biperiden, Orphenadrine, Procyclidine
Anticholinergics are recommended as monotherapy or as adjuncts to Levodopa. These may be considered for initial therapy prior to dopaminergic therapy in younger patients if tremor is predominant. These act by inhibiting the effects of acetylcholine in the brain. Use is generally not recommended for elderly patients or those with cognitive problems. Anticholinergics relieve symptoms of tremor in Parkinson’s disease but have little effect on bradykinesia. Benztropine and Trihexyphenidyl are most effective in patients with more prominent tremor than rigidity symptoms. Only 50% of patients respond to treatment with 30% improvement. Anticholinergic side effects limit their use.
Others
Amantadine
Amantadine is recommended as monotherapy or as an adjunctive therapy to an anticholinergic or Levodopa. This is a weak dopamine agonist with some antimuscarinic activity. This manages Parkinson’s disease in early stages when symptoms are mild. Amantadine relieves symptoms of bradykinesia, rigidity, and tremor. Amantadine may also improve dyskinesia. The effects wear off after several months of treatment and effectiveness may return after brief withdrawal.
Apomorphine
Intermittent Apomorphine injections may be used to reduce off time in people with Parkinson’s disease with severe motor complications. Continuous subcutaneous infusions of Apomorphine may be used to reduce off time and dyskinesia in people with Parkinson’s disease with severe motor complications. The initiation should be restricted to expert units with facilities for appropriate monitoring.
Istradefylline
Istradefylline is an oral adenosine A2A receptor antagonist approved by the US FDA as an adjunct treatment for ‘wearing off’ symptoms. A trial showed a decrease in the ‘wearing off’ time by approximately 1 hour compared to 15 minutes with a placebo.
TREATMENT OF NEUROLOGICAL AND PSYCHIATRIC COMPLICATIONS OF PARKINSON’S DISEASE
Parkinson’s Disease Dementia (PDD)
Stop the current drug that may aggravate the condition. Anticholinergic drugs used for treating motor symptoms of Parkinson’s disease may worsen cognition as well as psychotic symptoms. Rivastigmine is the only cholinesterase inhibitor approved for Parkinson’s disease dementia. This acts by inhibiting both acetylcholinesterase and butyrylcholinesterase. Rivastigmine has significant effects on cognitive symptoms and global function in patients with Parkinson’s disease dementia. This may improve behavior and activities of daily living. Donepezil may be considered in Parkinson’s disease dementia. The use of cholinesterase inhibitors has a potential risk of exacerbating motor symptoms.
Psychosis
Psychosis is often drug-induced. Reduce the dose or stop the offending drug. Clozapine may be added to current therapy. Quetiapine, but not Olanzapine, may also be considered. Pimavanserin has been recently approved for the treatment of hallucinations and delusions associated with Parkinson’s disease psychosis.
Depression
Optimize the current drug therapy. Selective serotonin reuptake inhibitors (SSRI), selective serotonin-norepinephrine reuptake inhibitors, and multimodal antidepressants are efficacious and well-tolerated options. Sertraline is the best-tolerated SSRI for Parkinson’s disease patients based on Delphi Consensus of Experts in Psychiatry, Neurology, and Geriatrics 2017. Other medications that can be used are Desvenlafaxine, Duloxetine, Mirtazapine, Venlafaxine and Vortioxetine. Non-ergot dopamine receptor agonists, such as Pramipexole and Ropinirole, are effective for treating PD-related depression.
Orthostatic Hypotension
Avoid factors that may trigger or worsen the condition (eg large meals, alcohol intake, warm environment, diuretics, antihypertensive drugs). In symptomatic patients, increase salt intake. The use of elastic stockings, or head-up tilt at night may be advised. Peripheral alpha-adrenergic agonist may increase the standing blood pressure. Consider Fludrocortisone, since it enhances renal sodium reabsorption and has alpha-adrenoreceptor sensitizing properties.
Urinary Incontinence
Avoid coffee and limit water intake before bedtime. A peripherally acting anticholinergic drug may be added to current therapy.
Gastrointestinal Motility Problems
Patients with Parkinson’s disease commonly develop constipation and reduced gastric motility. Advise the patient on diet, use of laxatives, and other measures to improve gastrointestinal motility. Patients on dopaminergic therapy frequently experiences gastrointestinal adverse effects (eg anorexia, nausea, and vomiting). Reduce the dose or stop current drugs with anticholinergic effects. May add Domperidone to current therapy.
Erectile Dysfunction
Consider the use of Sildenafil for erectile dysfunction.
Nonpharmacological
Supportive Treatment
Support groups offer psychosocial help to patients and families. Psychiatric counseling may be done to counsel the patient and families on how to cope with the illness. Legal counseling and financial counseling may also be done. Occupational counseling is done to counsel on the adaptations that may be needed to ensure productivity at work.
Exercise
 Parkinsons Disease and Dementia_Management 3
Parkinsons Disease and Dementia_Management 3Exercise may improve function, prevent falls, and improve mobility. Upright posture and gait training may be done. Extension exercises of the neck, trunk, and legs may be done by a formal exercise program where home exercises are performed daily. Refresher exercise may be done every 6-12 months.
Nutrition
Gastrointestinal musculature impairment may cause swallowing and chewing difficulties. Gastrointestinal disturbances due to prescribed medications may occur. Assist the patient in maintaining proper nutritional status through a balanced diet and good eating habits. Nutritional supplements may be given if required.
Fall Prevention
Slowness of gait, poor postural reflexes, involuntary movements, and orthostatic hypotension contribute to falls. Prevent falls by wearing rubber-soled shoes, removing throw rugs at home, and adjusting pharmacological therapy if required.
Management of Sleep Disturbances
Sleep disturbances occur due to the proximity of the substantia nigra to sleep and arousal centers in the brain stem. Manage sleep disturbances by medication adjustment, dietary modifications, sleep hygiene practices, or referral to a physician with specialized training in sleep physiology.
Speech Therapy
 Parkinsons Disease and Dementia_Management 4
Parkinsons Disease and Dementia_Management 4Speech therapy may help correct pharyngeal musculature impairment that may cause speech and swallowing difficulty. This may improve volume of speech and swallowing when administered with oral Levodopa.
Patient Education
 Parkinsons Disease and Dementia_Management 5
Parkinsons Disease and Dementia_Management 5Educate the patient on the nature of the illness and its treatment.
Surgery
Neurosurgery
Neurosurgery is considered in patients unresponsive to pharmacological therapy.
Pallidotomy
Unilateral pallidotomy has been shown to be effective in treating symptoms of dyskinesia when administered with oral Levodopa. This is unfavorable because of its irreversible nature.
Deep Brain Stimulation (DBS)
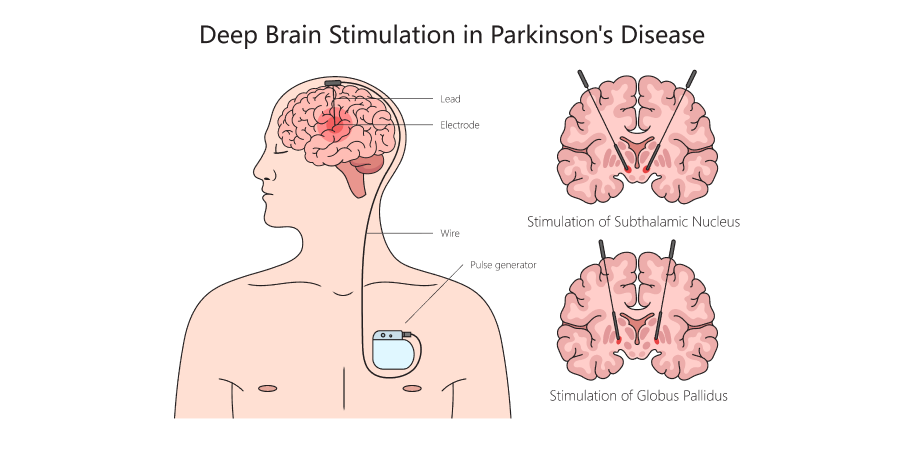 Parkinsons Disease and Dementia_Management 6
Parkinsons Disease and Dementia_Management 6Deep brain stimulation using implanted pulse generators in precise brain locations may be performed with specific indication. Both subthalamic nuclei (STN) and globus pallidus pars interna deep brain stimulation has shown efficacy in the management of Parkinson’s disease general/systemic motor symptoms (eg motor fluctuations, dyskinesia) when administered with oral Levodopa. Thalamic stimulation may be considered as an option in people with Parkinson’s disease who predominantly have severe disabling tremor and where subthalamic nuclei stimulation cannot be performed. Good candidates for deep brain stimulation include patients whose motor symptoms are not well-controlled by medications or who cannot tolerate side effects of medications and those who do not have significant active psychiatric or cognitive problems. Infection is the most commonly reported side effect of deep brain stimulation.