
Introduction
Vaginitis is inflammation in the walls of the vagina commonly caused by infections, hormonal changes, or irritants. Altered vaginal discharge in women of reproductive age may be secondary to non-sexually transmitted infections (STIs) (eg bacterial vaginosis [BV], vulvovaginal candidiasis [VVC]), STIs (eg Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, herpes simplex virus), or non-infective causes (eg foreign bodies, cervical polyps or ectopy, genital tract malignancy, fistulas, allergies). The most common causes of vaginitis are trichomoniasis, bacterial vaginosis and vulvovaginal candidiasis.
Please see Chlamydia - Uncomplicated Anogenital Infection, Genital Herpes, and Gonorrhea – Uncomplicated Anogenital Infection disease management charts for further information.
Epidemiology
Vaginitis is a common condition affecting millions of women worldwide, especially those of reproductive age and during hormonal changes such as pregnancy and menopause.
Trichomoniasis is the most common non-viral sexually transmitted infection globally, with about 153 million cases reported. Among women aged 40 years and older, the overall prevalence is about 11% and is higher in those with other sexually transmitted infections, including human immunodeficiency virus (HIV).
Bacterial vaginosis has an estimated global prevalence of 23-29% among women of reproductive age but occurs more commonly in low-resource settings and areas with limited healthcare access. The prevalence is similar in both pregnant and non-pregnant women. This is more common in women who are Black, who smoke and use vaginal douches or other intravaginal products. The prevalence of bacterial vaginosis varies widely by region, reaching about 50% in some areas of South Africa but only around 15% in Nigeria. Rates are moderate in South and Southeast Asia, Latin America, and the Caribbean and lowest in Europe.
Vulvovaginal candidiasis affects about 70-75% of women at one point or multiple times during their lifetime.
Etiology
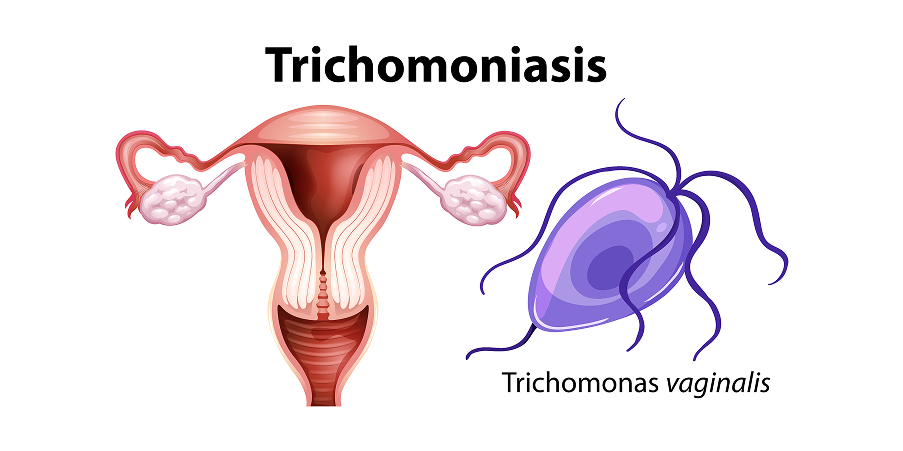
Trichomoniasis
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 1
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 1
Trichomoniasis is caused by Trichomonas vaginalis, a flagellated protozoan. This is almost always sexually transmitted and considered the most common non-viral sexually transmitted infections (STIs). Most infections present with minimal or no symptoms and, if left untreated, may last for months to years.
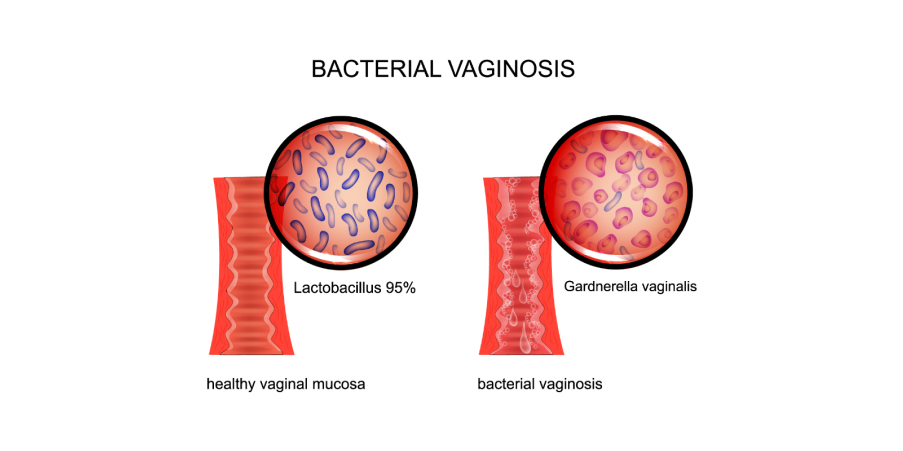
Bacterial Vaginosis (BV)
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 2
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 2Bacterial vaginosis results from the overgrowth of anaerobic bacteria (eg Prevotella sp, Mobiluncus sp, Gardnerella vaginalis, Atopobium vaginae, Ureaplasma sp, Mycoplasma hominis) replacing the normal hydrogen peroxide-producing Lactobacillus sp in the vaginal flora. The presence of Gardnerella alone is not conclusive to diagnose bacterial vaginosis because it is a commensal organism in some asymptomatic women and the most common cause of vaginitis, vaginal discharge, or malodor. This may be accompanied by pruritus or irritation around the vagina and a burning sensation during urination. Bacterial vaginosis is considered to be sexually associated but not truly sexually transmitted and may coexist with trichomoniasis and other sexually transmitted infections.
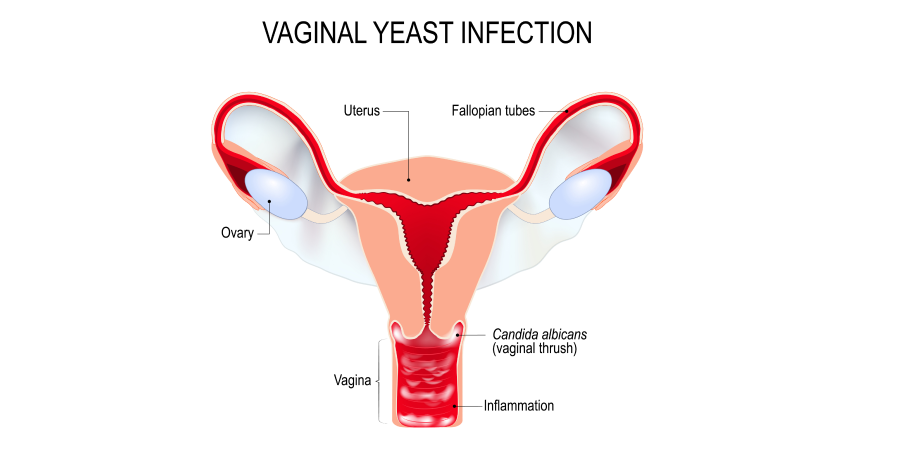
Vulvovaginal Candidiasis (VVC)
 Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 3
Vaginitis Trichomoniasis, Candidiasis, Bacterial Vaginosis_Disease Background 3Vulvovaginal candidiasis is caused by an overgrowth of yeasts, where about 90% of cases are secondary to Candida albicans. Though sexually associated, it is not a sexually transmitted infection.
Pathophysiology
Vaginitis is more common during the reproductive years because estrogen increases glycogen in the vaginal mucosa, which supports Lactobacillus growth and maintains an acidic vaginal pH that helps prevent infection. Changes in hormones (eg during pregnancy, menopause, breastfeeding), menstruation, antibiotic use, douching, and unprotected intercourse can disrupt this balance and alter normal vaginal flora. The immune response also plays an important role in the pathophysiology of vaginitis, as an excessive or inappropriate reaction can worsen inflammation and contribute to the persistence of chronic symptoms.
Risk Factors
Trichomoniasis caused by T vaginalis is significantly associated with older age, lower educational attainment, unprotected intercourse, lower socioeconomic status, and having two or more sexual partners in the past year.
Risk factors for bacterial vaginosis include sexual activity, especially with new, female, or multiple partners and inconsistent condom use. Additional contributing factors include vaginal douching, recent antibiotic therapy, smoking, and hypoestrogenism, all of which can disrupt normal vaginal flora.
Vulvovaginal candidiasis (VVC) most commonly occurs when the vagina is exposed to estrogen (ie reproductive years, pregnancy) and may be precipitated by antibiotic, oral contraceptive, or corticosteroid use. Immunocompromised and diabetic women are also at risk. Immunocompetent patients without comorbidities with sporadic or infrequent VVC, mild to moderate VVC, and with C albicans infection are considered to have uncomplicated VVC. Immunocompromised or debilitated patients with comorbidities with recurrent (4 episodes/year), severe, or non-albicans VVC are classified as having complicated VVC.