
Introduction
The definition of hypertension is based on office or in-hospital blood pressure (BP) measurements. Ambulatory BP monitoring is preferred over routine BP measurement in predicting the outcome of pregnancy.
Hypertension in pregnancy is defined as a systolic BP (SBP) of ≥140 mmHg or a diastolic BP (DBP) of ≥90 mmHg, or both, based on at least two measurements ≥4 hours apart. The diagnosis of severe hypertension is made when SBP is ≥160 mmHg and/or DBP is ≥110 mmHg, and mild when BP is 140-159/90-109 mmHg. The measurement should be repeated after 15 minutes for confirmation of severe hypertension.
Epidemiology
Hypertension is the most frequently occurring medical condition during pregnancy. The estimated prevalence of hypertension among pregnant women is approximately 6-8%. Chronic hypertension is present in about 1.5% of pregnancies. Pregnant individuals with hypertension have a 5-fold increased risk of developing preeclampsia. Preeclampsia is a major contributor to maternal and perinatal morbidity and mortality. In developed countries, the prevalence is higher, ranging from about 6% to 8%.
Pathophysiology
The exact cause of preeclampsia and eclampsia remains unknown; however, its pathophysiology is associated with immunologic and angiogenic abnormalities within the placenta. Abnormal trophoblastic invasion of the decidual spiral arteries and myometrium leads to reduced uteroplacental perfusion, resulting in placental ischemia and oxidative stress. This process contributes to inadequate development of the fetoplacental vasculature and the release of angiogenic factors into the maternal circulation, ultimately causing hypertension and proteinuria.
Risk Factors
Risk Factors for Preeclampsia
 Hypertension in Pregnancy_Disease Background 1
Hypertension in Pregnancy_Disease Background 1
Identify at-risk patients with normal BP in early gestation for close monitoring to prevent preeclampsia.
Moderate risk for preeclampsia is defined as the presence of ≥2 of the following: First pregnancy; extremes of maternal age (<20 years or ≥40 years); obesity (BMI ≥35 kg/m2) at first visit or excessive weight gain >1 kg/week; family history of preeclampsia or eclampsia; pregnancy interval >10 years; multifetal pregnancy; and history of placental abruption, intrauterine growth restriction (IUGR) or unexplained stillbirth.
High risk for preeclampsia is defined as the presence of any one of the following: History of preeclampsia or eclampsia; chronic hypertension; history of hypertension in previous gestation before week 34; pre-existing medical conditions (eg type 1 or type 2 DM, collagen vascular diseases, chronic kidney disease, renal vascular or parenchymal diseases); autoimmune disease (eg SLE or antiphospholipid antibody syndrome); and assisted reproductive therapy in current pregnancy.
Risk Factors for Superimposed Preeclampsia
Risk factors for superimposed preeclampsia include renal insufficiency; history of hypertension >4 years; hypertension in previous pregnancy; and an increase in ALT and AST to abnormal levels.
Classification
Categories of Hypertension in Pregnancy
Gestational age is central to the classification of hypertensive disorders of pregnancy as vascular and hemodynamic changes cause the BP to fall in early pregnancy, reach a nadir in the second trimester and return to baseline by the end of the third trimester.
Chronic (Pre-existing) Hypertension
Chronic hypertension is defined as BP measurement of ≥140/90 mmHg on two occasions prior to pregnancy or before 20 weeks of gestation; this usually persists beyond 6 weeks postpartum. Proteinuria may be present. The risk of developing preeclampsia is increased.
Gestational Hypertension
Gestational hypertension refers to women with previously normal BP who develop hypertension without proteinuria or target organ damage (TOD) after 20 weeks of gestation. This may correspond to the preproteinuric phase of preeclampsia or recurrence of chronic hypertension abated in midpregnancy. A diagnosis that is made retrospectively if preeclampsia is not present at the time of delivery and the BP returns to normal by 6 weeks postpartum. This may progress to preeclampsia. Transient gestational hypertension is usually detected in the clinic but settles with repeated BP measurements over several hours; it carries a 40% risk of progressing to true gestational hypertension or preeclampsia, thus necessitating careful follow-up.
Preeclampsia
 Hypertension in Pregnancy_Disease Background 2
Hypertension in Pregnancy_Disease Background 2Preeclampsia is the term used to describe a condition presenting as de novo hypertension after 20 weeks of gestation (gestational hypertension), with one or more of the following:
- Proteinuria: A 24-hour urine level ≥300 mg, protein/creatinine ratio ≥30 mg/mmol, albumin/creatinine ratio ≥8 mg/mmol or ≥2+ protein on urine dipstick
- Hematologic disorder: Hemolysis, thrombocytopenia (platelet count <100 × 109/L) or coagulopathy
- Liver problems: Elevated liver enzymes with or without severe epigastric or right upper quadrant pain
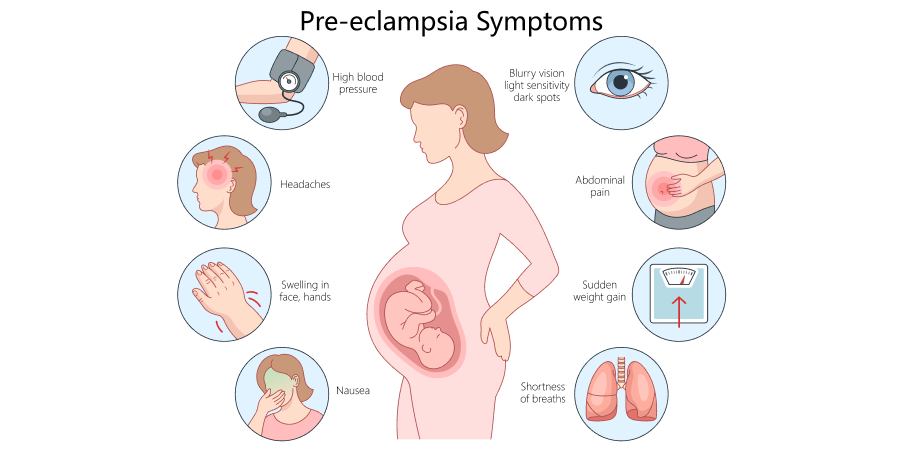
- Neurologic signs: Severe headache, altered mental status, persistent visual disturbances (scotoma), blindness, hyperreflexia with clonus, seizures (eclampsia), or stroke
- Renal insufficiency: Oliguria or serum creatinine >1-1.1 mg/dL or increased to twice the normal concentration without other renal disease
- Pulmonary edema
- Uteroplacental dysfunction: Fetal growth restriction, placental abruption, stillbirth, or abnormal umbilical artery Doppler waveform analysis
Eclampsia
 Hypertension in Pregnancy_Disease Background 3
Hypertension in Pregnancy_Disease Background 3Eclampsia is a severe convulsive manifestation of the hypertensive disorders of pregnancy that is not caused by drug use, epilepsy, intracranial hemorrhage, or cerebral arterial ischemia and infarction. There is a new onset of seizures or coma in a patient with preeclampsia. This can occur without warning signs or symptoms, and both preeclampsia and eclampsia can happen before, during, or after labor.
Unclassifiable Antenatal Hypertension
Unclassifiable antenatal hypertension is hypertension that is first noted after 20 weeks of gestation, requiring re-evaluation at or after 6 weeks postpartum in order to differentiate chronic from gestational hypertension. If hypertension resolves, it is reclassified as gestational hypertension, but if it persists, it is reclassified as chronic hypertension.