
Introduction
 Hyponatremia_Disease Background 1
Hyponatremia_Disease Background 1Hyponatremia is serum sodium concentration <135 mEq/L due to the failure of normal water excretion. Severe hyponatremia is when there is <120 mEq/L serum sodium concentration. Hyponatremia increases the risk of falls and osteoporosis, and in severe cases it can be associated with mental state changes, including the risk of coma and seizures.
Epidemiology
Hyponatremia is the most common body fluid disorder and electrolyte imbalance encountered in clinical practice. This accounts for 15-30% of emergency admissions in hospitals and is associated with increased morbidity, mortality, and length of hospital stay in patients presenting with a range of conditions. Advancing age is associated with an increased risk of hyponatremia, with a higher prevalence observed in older women than in older men.
Studies across Asian medical centers demonstrate that 25-30% of elderly inpatients present with hyponatremia. A Taiwanese emergency department study reported a 4% prevalence of hyponatremia, with hypovolemic hyponatremia due to gastroenteritis being the primary cause.
Etiology
The most common causes of hyponatremia are medication effects, fluid retention, and the syndrome of inappropriate antidiuretic hormone secretion (SIADH).
Pathophysiology
The osmolality (total concentration of solutes in water) of plasma plays a role in the pathophysiology of hyponatremia. The arginine vasopressin (antidiuretic hormone [ADH]) system and strict thirst regulation help maintain plasma osmolality. An increase in plasma osmolality leads to ADH secretion and water retention, which decreases serum osmolality. A decrease in plasma osmolality decreases ADH, which will result in diuresis of free water and a return to homeostasis. Hyponatremia is usually associated with disturbance in the ADH that governs water balance. This is a disorder of water imbalance where there is a relative excess of body water compared to total body sodium and potassium content due to impaired renal water excretion.
Risk Factors
Hyponatremia is associated with several medications and substances, including 3,4-methylenedioxymethamphetamine (MDMA or “Ecstasy”), angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), anticonvulsants, intravenous cyclophosphamide, oxytocin, and thiazide diuretics. Acute hyponatremia is also commonly seen in postoperative patients and individuals undergoing colonoscopy preparation.
Classification
Classification Based on Duration
Acute Hyponatremia
Hyponatremia that has developed over a period of <48 hours or onset of <3 days is classified as acute. This usually results from parenteral fluid administration in post-op patients and from self-induced water intoxication (as seen in competitive runners, extreme polydipsia in mentally ill patients, and Ecstasy users). The main pathologic consequence of acute hyponatremia is the development of cerebral edema that may lead to raised intracranial pressure, cerebral herniation, hypoxia, and even death.
Chronic Hyponatremia
Hyponatremia that has been present for ≥48 hours or whose duration is unclear is classified as chronic. This is due to the presence of cerebral adaptive mechanisms, and many patients exhibit no apparent ill effects despite severe biochemical hyponatremia. The initial adaptive mechanism is the loss of intracerebral fluid with depletion of sodium and potassium to prevent cerebral edema and gain of water.
Classification Based on Severity or Degree of Hyponatremia
Mild Hyponatremia
A serum sodium concentration of 130-134 mEq/L is classified as mild.
Moderate Hyponatremia
A serum sodium concentration of 120-129 mEq/L is classified as moderate.
Severe Hyponatremia
A serum sodium concentration of <120 mEq/L is classified as severe. This is termed "profound hyponatremia" by the 2014 European Society of Intensive Care Medicine (ESICM) - European Society of Endocrinology (ESE) - European Renal Association (ERA) guideline.
Classification Based on Tonicity
Hypotonic Hyponatremia
Hypotonic hyponatremia has a serum osmolality of <275 mOsm/kg H₂O. The most common cause of hypotonic hyponatremia is impairment in urinary dilution mediated by vasopressin. Patients may be hypovolemic, euvolemic, or hypervolemic.
Isotonic Hyponatremia
Isotonic hyponatremia has a serum osmolality of 275-295 mOsm/kg H₂O. This can be associated with pseudohyponatremia.
Hypertonic Hyponatremia
Hypertonic hyponatremia has a serum osmolality of >295 mOsm/kg H₂O. This is a translocational hyponatremia most commonly seen in hyperglycemia.
Classification Based on Extracellular Volume Status
 Hyponatremia_Disease Background 2
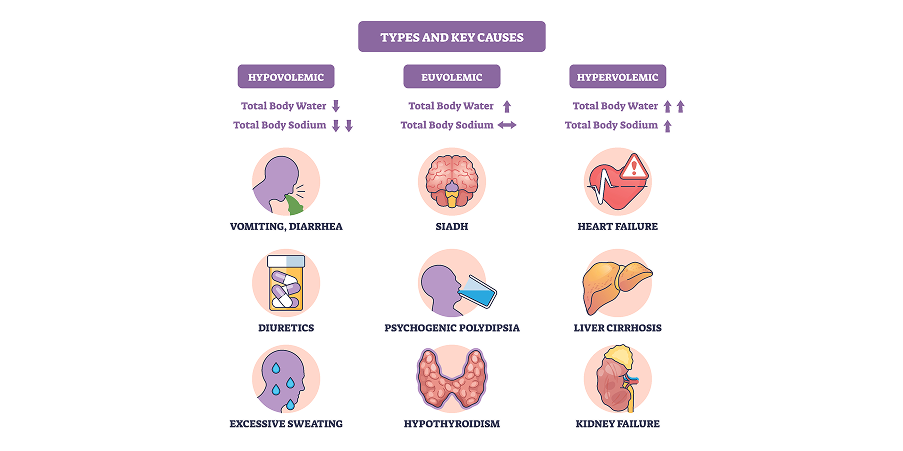
Hyponatremia_Disease Background 2Hypovolemic Hyponatremia
Hypovolemic hyponatremia is a decreased total body water with a greater decrease in sodium level. Extracellular fluid losses can occur from the kidneys, the gastrointestinal tract, or the skin. The most common cause is thiazide diuretic therapy. Other causes of hypovolemic hyponatremia are Addison’s disease and cerebral salt wasting. Signs and symptoms associated with volume depletion are dry mucous membranes, decreased skin turgor, vomiting, diarrhea, tachycardia, hypotension, and elevated blood urea nitrogen-to-creatinine ratio and uric acid level. Urinary sodium is usually <20 mEq/L unless the kidney is the site of sodium loss.
Euvolemic Hyponatremia
Euvolemic hyponatremia is an increased total body water with a normal sodium level. This accounts for the majority of hyponatremia cases. This is most commonly caused by the syndrome of inappropriate antidiuretic hormone secretion (SIADH). Other causes of euvolemic hyponatremia are hypothyroidism, primary polydipsia, and glucocorticoid deficiency. Clinical signs depend on the underlying illness. Diagnostic lab findings include a low serum uric acid level, a normal blood urea nitrogen-to-creatinine ratio, and a spot urinary sodium of >20 mEq/L.
Hypervolemic Hyponatremia
Hypovolemic hyponatremia is an increased total body water compared with sodium that occurs when the kidneys cannot excrete water efficiently. Common causes of hypervolemic hyponatremia include heart failure, liver cirrhosis, and kidney injury. Clinical signs include peripheral edema, ascites, raised jugular venous pressure, pulmonary edema, and an underlying illness. Useful diagnostic lab findings are elevated plasma levels of brain natriuretic peptide and spot urine of <20-30 mEq/L.