
Clinical Presentation
Signs and Symptoms
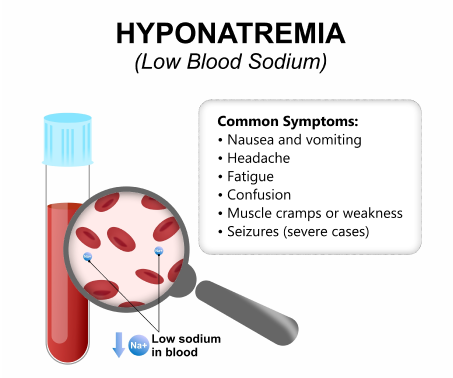
Patients with hyponatremia are commonly asymptomatic, and it is only an incidental finding. A gradual decrease in sodium usually shows minimal symptoms, whereas rapid decreases manifest severe symptoms. Severe symptoms are due to brain edema and increased intracranial pressure.
 Hyponatremia_Initial Assesment 1
Hyponatremia_Initial Assesment 1Mild to moderate symptoms that are relatively non-specific and occur most commonly in patients with severe chronic hyponatremia are the following: Headache, fatigue, lethargy, nausea and vomiting, dizziness, gait disturbances, forgetfulness, confusion, and muscle cramps. Severe symptoms include seizures, obtundation, coma, and respiratory arrest. Acute intervention is needed if the following symptoms occur: Polydipsia, muscle cramps, headaches, falls, confusion, altered mental status, obtundation, coma, and status epilepticus.
History
 Hyponatremia_Initial Assesment 2
Hyponatremia_Initial Assesment 2When obtaining the patient's history, inquire about possible causes of hyponatremia. Assess for a history of cardiac, cancer, pulmonary, endocrine, gastrointestinal, neurologic, and renal diseases. Determine whether the patient has experienced electrolyte-rich fluid losses, such as from vomiting, diarrhea, or diuretic therapy. Ask about dietary habits, including low protein intake and/or excessive fluid intake. Review all medications (eg diuretics, Carbamazepine, selective serotonin reuptake inhibitors). Assess for alcohol (eg beer) and illicit drug use (eg 3,4-methylenedioxymethamphetamine/”Ecstasy”). For athletes, inquire about training regimens because high-endurance activities can cause hyponatremia. Determine whether the patient has undergone any very recent surgical procedures.
Physical Examination
During the physical examination, assess for signs of extracellular volume depletion (eg decreased skin turgor, low jugular venous pressure, or orthostatic or persistent hypotension indicating hypovolemia). Evaluate for signs of peripheral edema and/or ascites that can be due to heart failure, cirrhosis, or renal failure. Look for signs that are suggestive of adrenal insufficiency or hypothyroidism.
Diagnosis or Diagnostic Criteria
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
 Hyponatremia_Initial Assesment 3
Hyponatremia_Initial Assesment 3
The diagnosis of SIADH is based on the clinical euvolemic state with low serum sodium and osmolality and raised urine sodium and osmolality.
Essential Diagnostic Criteria Based on Bartter and Schwartz
- Hyposmolality: plasma osmolality <275 mOsm/kg
- Inappropriate urinary concentration (UOsm >100 mOsm/kg)
- Clinically euvolemic patient
- Elevated urinary sodium (>20-40 mEq/L), with normal salt and water intake
- Hypothyroidism and glucocorticoid deficiency excluded particularly in patients with neurosurgical conditions
- No recent use of diuretic agents
- Absence of heart failure, cirrhosis or advanced kidney disease
Supplemental Criteria
- Serum uric acid <4 mg/dL
- Serum urea <21.6 mg/dL
- Failure to correct hyponatremia after 0.9% saline infusion
- Correction of hyponatremia through fluid restriction
- Fractional sodium excretion >0.5%
- Fractional urea excretion >55%
- Fractional uric acid excretion >2%
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) can occur due to medications, malignancy (eg small cell lung cancer), pulmonary disease, or any disorder involving the central nervous system (eg subarachnoid hemorrhage). This is a nonspecific but potent stimulus for vasopressin secretion. Frequent causes of SIADH in hospitalized patients are general anesthesia, nausea, pain, stress, and a variety of drugs.
Hyponatremia that resulted from ADH-induced retention of ingested or infused water may result from increased release by the pituitary gland or from ectopic production. This may also result from increased activity of the vasopressin in the collecting duct or from a gain-of-function mutation in its type 2 receptor. The choice of therapy depends on several factors, such as the degree of hyponatremia, presence or absence of symptoms, and urine osmolality. Fluid restriction of 800-1,200 mL/24 hr is the mainstay of treatment.